Department of Otorhinolaryngology, Head and Neck Surgery, Inselspital, University Hospital and University of Bern.
ARTORG Center for Biomedical Engineering Research, University of Bern, Bern, Switzerland.
Otol Neurotol. 2021 Mar 1;42(3):e341-e347. doi: 10.1097/MAO.0000000000002992.
We aimed to investigate the effect of the head excursion angle on the success of the Sémont Maneuver (SM).
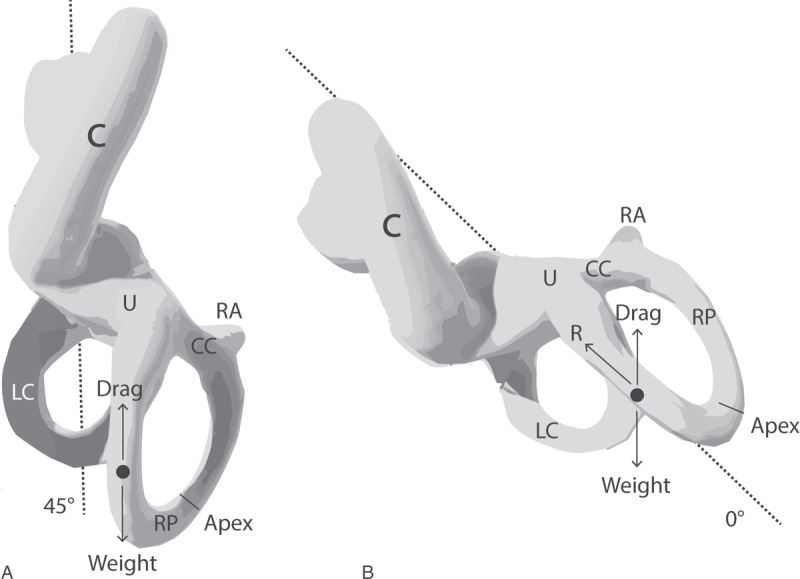
SM is performed with the head turned by 45 degrees toward the unaffected ear. In clinical routine, it is unlikely that physicians can turn the head to a position of exactly 45 degrees. Moreover, it is unclear how possible deviations from 45 degrees would affect the outcome with SM.
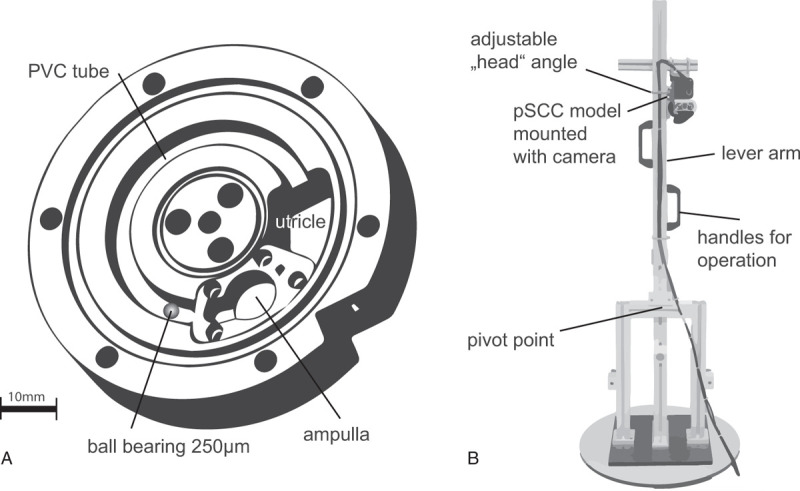
We used an in vitro model (upscaled by ×5) of a posterior semicircular canal with canalithiasis to study head excursion angles (0-75 degrees) and minimum waiting times in SM. Additionally, we measured actual head excursion angles performed by trained physicians during SM on a healthy subject.
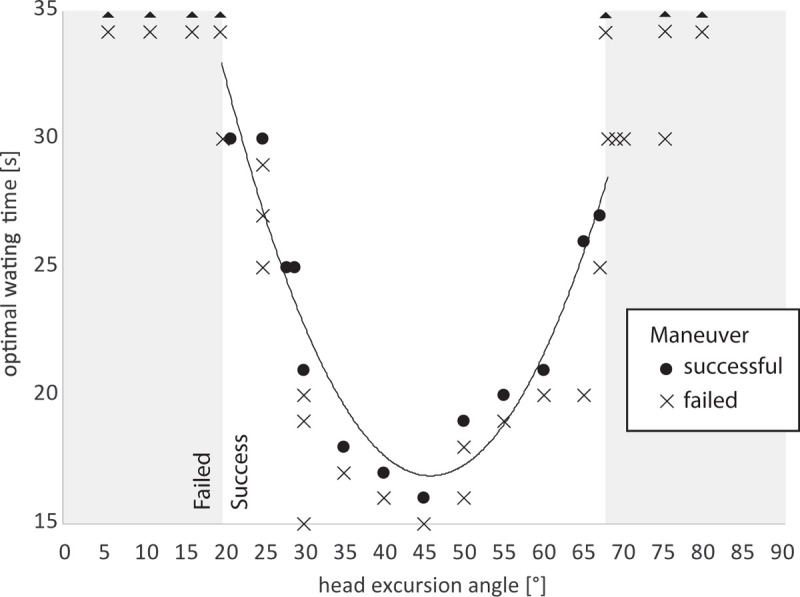
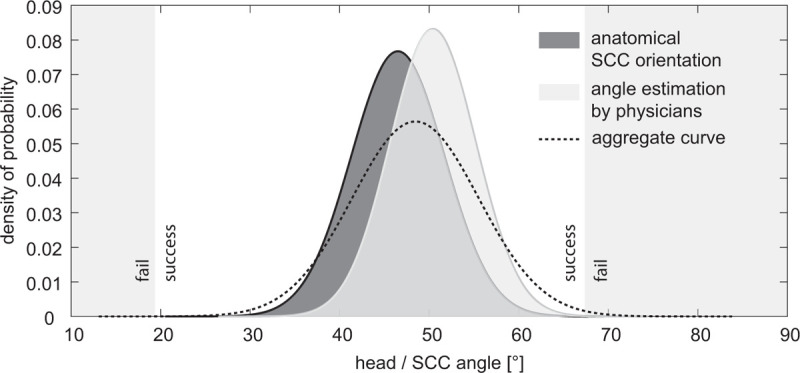
Successful canalith repositioning to the utricle was possible at head excursion angles between 21 and 67 degrees. Waiting time increased from 16 to 30 seconds with increasing deviation from 45 degrees. Angles larger than 67 degrees or smaller than 21 degrees did not lead to successful repositioning even after a waiting period of 5 minutes. Physicians set head excursion angles of 50 degrees ±SD 4.8 degrees while performing the SM.
Angular deviations up to ±20 degrees from the ideal SCC plane (45 degrees) still allows for successful SM. Although the tested physicians tended to underestimate the actual head excursion angle by 5 degrees (and more), the success of SM will not be affected provided that the waiting time is sufficiently long. Further, the results suggest that the Brandt-Daroff maneuver is a form of habituation training rather than a liberatory maneuver.
我们旨在研究头部摆动角度对 Sémont 手法(SM)成功的影响。
SM 是在头部向未受影响的耳朵转动 45 度的情况下进行的。在临床常规中,医生不可能将头部转到完全 45 度的位置。此外,不清楚偏离 45 度的角度如何影响 SM 的结果。
我们使用一个带有结石的后半规管的体外模型(放大 5 倍)来研究头部摆动角度(0-75 度)和 SM 中的最小等待时间。此外,我们还测量了训练有素的医生在健康受试者中进行 SM 时的实际头部摆动角度。
在头部摆动角度为 21 度至 67 度之间,成功地将耳石重新定位到前庭。等待时间从 16 秒增加到 30 秒,与偏离 45 度的角度增加成正比。角度大于 67 度或小于 21 度,即使等待 5 分钟,也不会导致成功复位。医生在进行 SM 时设置的头部摆动角度为 50 度±SD 4.8 度。
与理想的 SCC 平面(45 度)相比,角度偏差高达±20 度仍可实现成功的 SM。尽管测试的医生往往会低估实际的头部摆动角度 5 度(甚至更多),但只要等待时间足够长,SM 的成功就不会受到影响。此外,结果表明 Brandt-Daroff 手法是一种习惯训练形式,而不是一种解放手法。