Department of Pulmonary Medicine, Erasmus Medical Center Rotterdam, Doctor Molewaterplein 40, 3015 GD Rotterdam, the Netherlands.; Erasmus MC Cancer Institute, Erasmus Medical Center Rotterdam, Doctor Molewaterplein 40, 3015 GD Rotterdam, the Netherlands.
Department of Thoracic Oncology, NKI-AVL, Amsterdam, the Netherlands.
EBioMedicine. 2020 Dec;62:103040. doi: 10.1016/j.ebiom.2020.103040. Epub 2020 Nov 7.
Combined immune checkpoint inhibitor (ICI) treatment targeting PD-1 and CTLA-4 was suggested to yield clinical benefit over chemotherapy in malignant pleural mesothelioma (MPM), whereas aPD-1 monotherapy failed to provide benefit in phase-III trials. Success of ICI depends on the presence and activation of tumor-specific T cells. Therefore, we investigated whether T-cell characteristics are underlying clinical efficacy of ICI treatment in MPM.
Comprehensive immune cell profiling was performed on screening and on treatment peripheral blood samples of mesothelioma patients treated with nivolumab (aPD-1) monotherapy (NCT02497508), or a combination of nivolumab and ipilimumab (aCTLA-4) (NCT03048474).
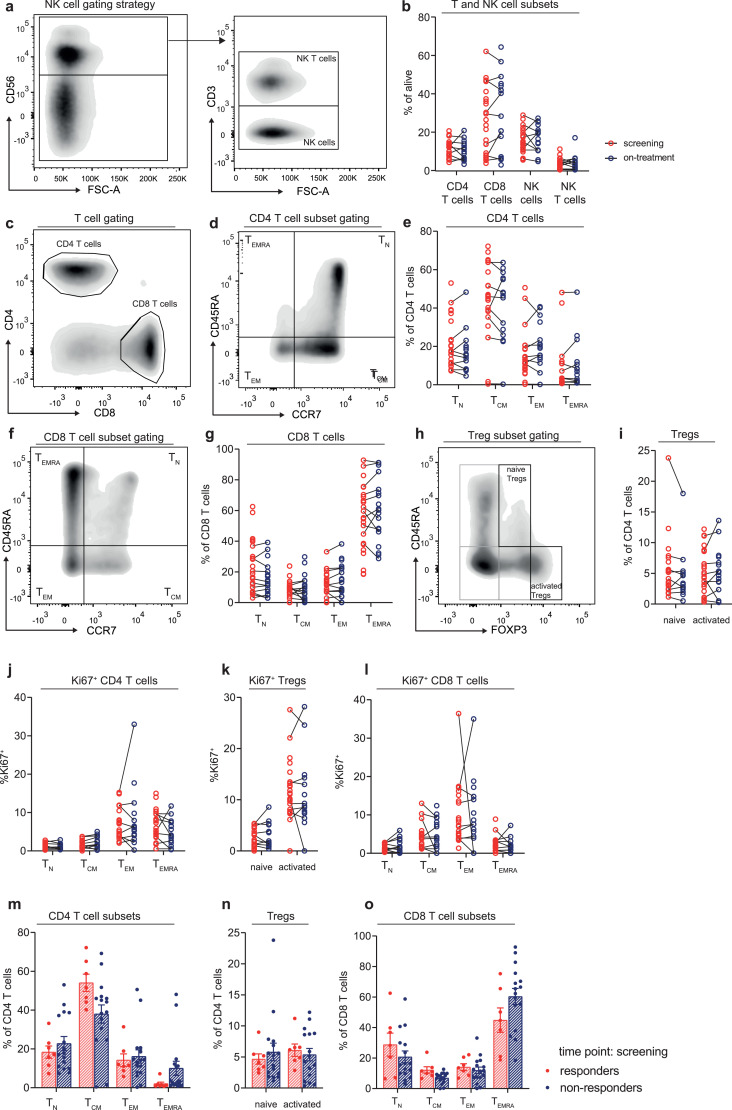
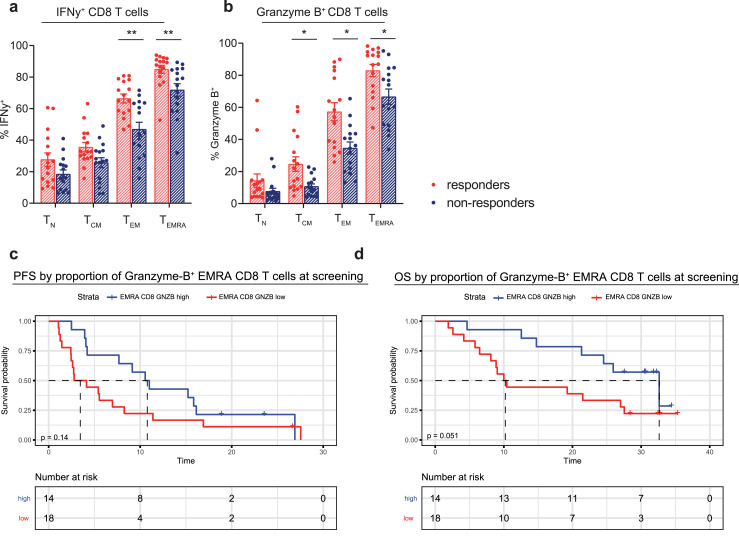
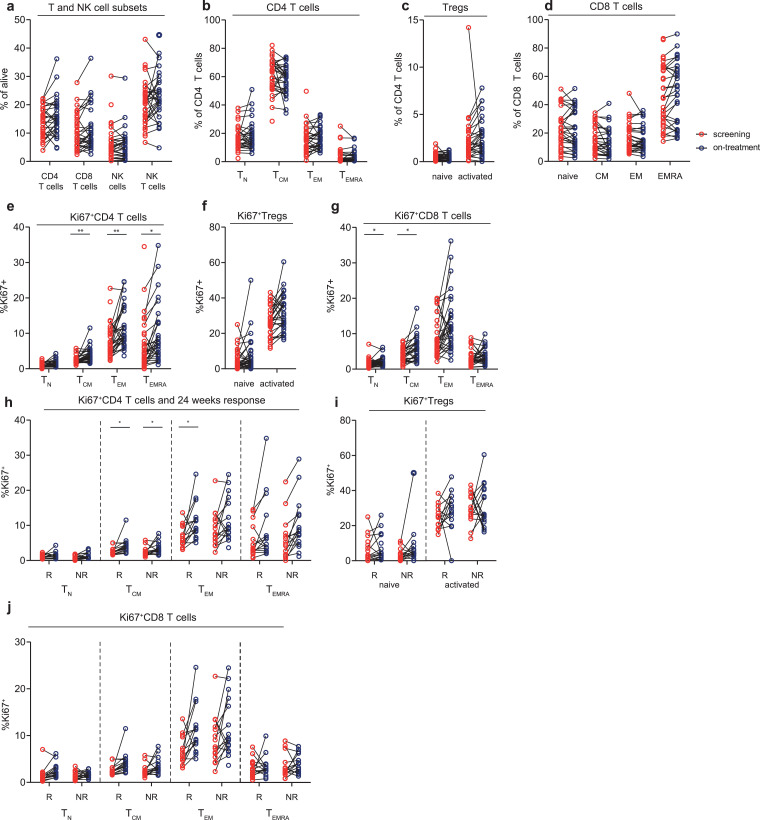
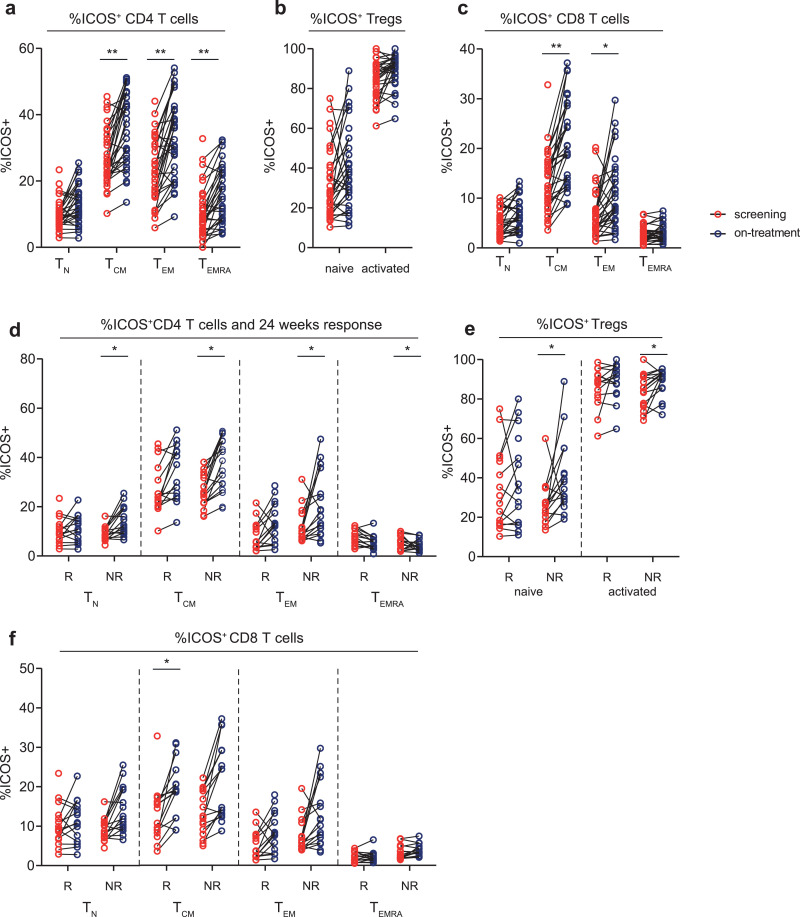
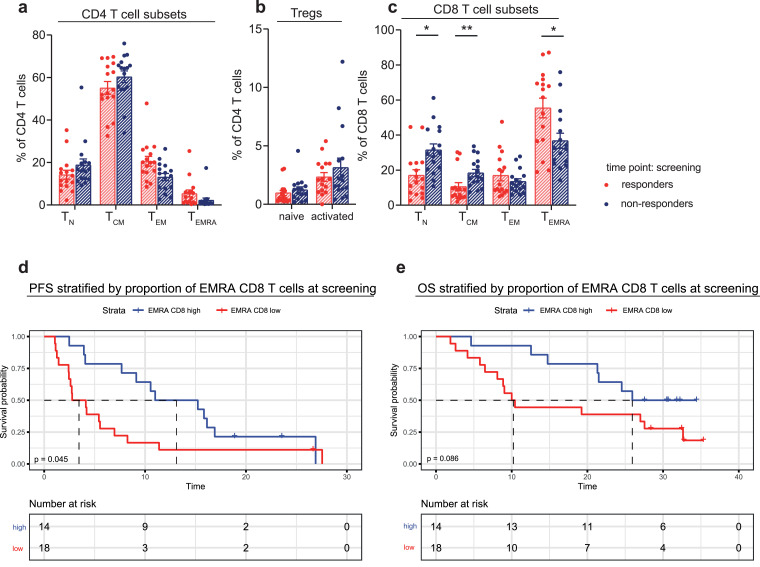
aPD-1/aCTLA-4 combination treatment induced a profound increase in proliferation and activation of T cells, which was not observed upon aPD-1 monotherapy. Moreover, patients that responded to combination treatment had low frequencies of naive CD8 T cells and high frequencies of effector memory CD8 T cells that re-expressed RA (TEMRA) at screening. The frequency of Granzyme-B and Interferon-γ producing TEMRAs was also higher in responding patients.
High proportions of TEMRAs and cytokine production by TEMRAs before treatment, was associated with a better clinical outcome. TEMRAs, which likely comprise tumor-specific T cells, tend to require blockage of both aPD-1 and aCTLA-4 to be reactivated. In conclusion, peripheral blood TEMRAs can play a key role in explaining and predicting clinical benefit upon aPD-1/aCTLA-4 combination treatment.
Bristol-Myers Squibb sponsored NivoMes and INITIATE clinical trials and provided study drugs. No external funding was applicable for the flow cytometric analyses of peripheral blood samples described in this manuscript.
联合免疫检查点抑制剂(ICI)治疗方案,针对 PD-1 和 CTLA-4,在恶性胸膜间皮瘤(MPM)中,与化疗相比,显示出临床获益,而抗 PD-1 单药治疗在 III 期临床试验中未能获益。ICI 的成功取决于肿瘤特异性 T 细胞的存在和激活。因此,我们研究了 T 细胞特征是否是 ICI 治疗 MPM 临床疗效的基础。
对接受纳武单抗(抗 PD-1)单药治疗(NCT02497508)或纳武单抗联合伊匹单抗(抗 CTLA-4)治疗(NCT03048474)的间皮瘤患者的筛选和治疗外周血样本进行全面免疫细胞分析。
aPD-1/aCTLA-4 联合治疗诱导 T 细胞增殖和激活显著增加,而 aPD-1 单药治疗则未观察到。此外,对联合治疗有反应的患者在筛选时具有较低的幼稚 CD8 T 细胞频率和较高的效应记忆 CD8 T 细胞频率,这些细胞重新表达 RA(TEMRA)。反应患者的 TEMRA 中颗粒酶-B 和干扰素-γ产生的频率也更高。
治疗前 TEMRA 的高比例和 TEMRA 产生细胞因子与更好的临床结局相关。TEMRA 可能包含肿瘤特异性 T 细胞,它们倾向于需要同时阻断 aPD-1 和 aCTLA-4 才能被重新激活。总之,外周血 TEMRA 可能在解释和预测 aPD-1/aCTLA-4 联合治疗的临床获益方面发挥关键作用。
百时美施贵宝赞助了 NivoMes 和 INITIATE 临床试验,并提供了研究药物。本手稿中描述的外周血样本的流式细胞术分析没有外部资金。