Center of Innovation in Long Term Services and Supports, Providence Veterans Affairs Medical Center, Providence, RI, USA.
College of Nursing, The Pennsylvania State University, University Park, PA, USA.
Clin Interv Aging. 2020 Nov 2;15:2053-2061. doi: 10.2147/CIA.S249284. eCollection 2020.
INTRODUCTION/BACKGROUND: Frailty identifies patients that have vulnerability to stress. Acute illness and hospitalization are stressors that may result in delirium and further accelerate the negative consequences of frailty.
The purpose of this study was to determine whether frailty, identified at hospital admission and as measured by a frailty index, is associated with incident delirium.
A retrospective, observational, cohort study was done at a Veterans hospital between January 2013 and March 2014. English-speaking patients over 55 years were eligible. Exclusion criteria included inability to complete baseline assessments due to pre-existing cognitive impairment, emergent surgery; and/or admission from a nursing home, pre-existing delirium, and those with psychiatric disease or substance use disorder.
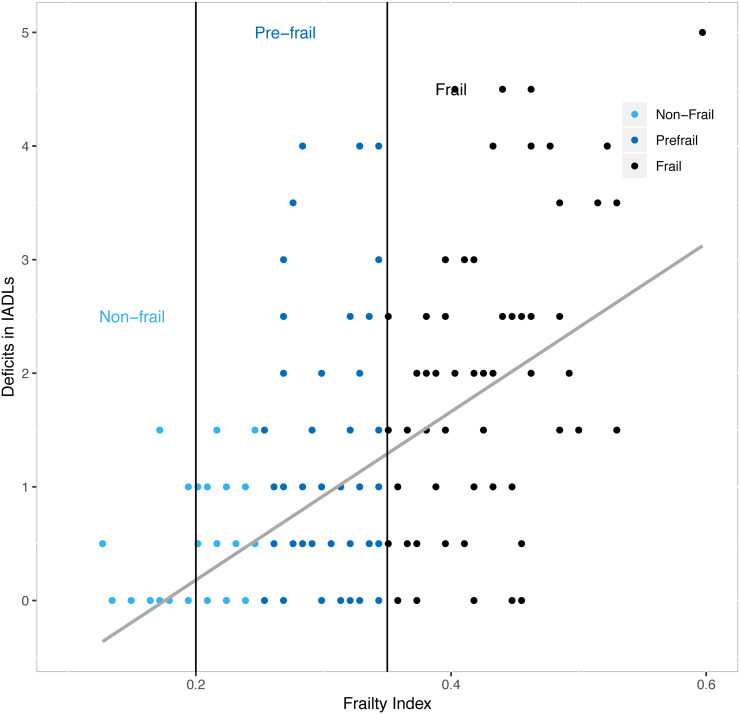
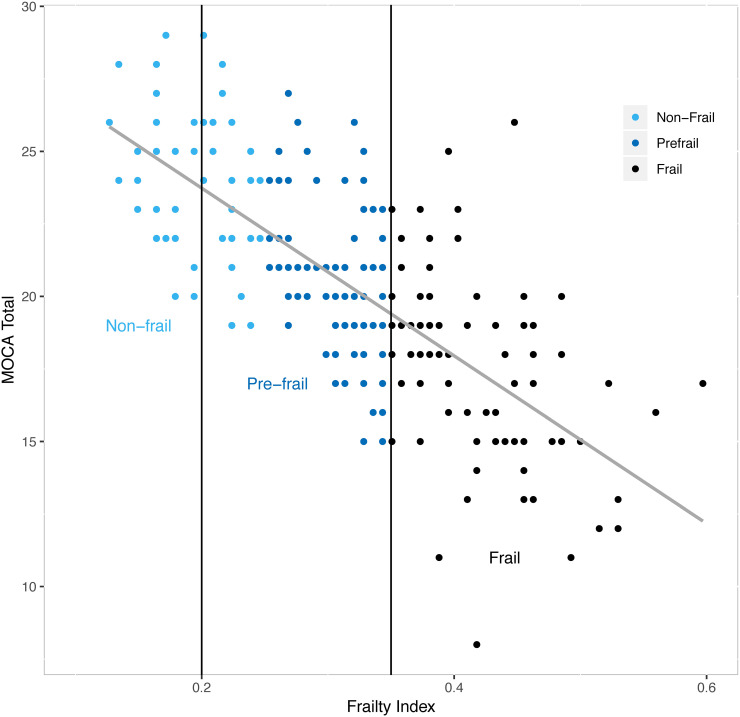
Frailty index (FI) variables included cognitive screening, physical function and comorbidities. The FI was calculated as a proportion of possible deficits (range 0 to 1; higher scores indicate increased frailty). Incident delirium was measured daily by an expert clinician interview.
A total of 247 patients were admitted and 218 met inclusion/exclusion criteria, with a mean age of 71.54 years (SD = 9.53 years) and were predominantly white (92.7%) and male (91.7%). Participants were grouped using FI ranges as non-frail (FI <0.25, n=56 (26%)), pre-frail (FI =0.25-0.35, n=86 (39%)), and frail (FI >0.35, n=76 (35%)). Pre-frailty and frailty were associated with incident delirium (non-frail: 3.6% vs pre-frail: 20.9% vs frail: 29.3%, =0.001) and total delirium days (mean day =non-frail 0.04 vs pre-frail 0.35 vs frail 0.57, =0.003). After adjustment for sociodemographic factors, pre-frail (adjusted OR=5.64, 95% CI: 1.23, 25.99) and frail status (adjusted OR=6.80, 95% CI: 1.38, 33.45) were independently associated with delirium.
This study demonstrates that a frailty index is independently associated with incident delirium and suggests that admission assessments for frailty may identify patients at high risk of developing delirium.
介绍/背景:衰弱确定了对压力敏感的患者。急性疾病和住院是应激源,可能导致谵妄,并进一步加速衰弱的负面后果。
本研究旨在确定入院时通过衰弱指数确定的衰弱与谵妄的发生是否相关。
这是一项在退伍军人医院进行的回顾性、观察性队列研究,时间为 2013 年 1 月至 2014 年 3 月。55 岁以上的英语患者有资格参加。排除标准包括由于先前存在的认知障碍、急诊手术;以及/或从疗养院入院、先前存在的谵妄、以及患有精神疾病或物质使用障碍的患者,由于基线评估无法完成。
衰弱指数(FI)变量包括认知筛查、身体功能和合并症。FI 按可能缺陷的比例计算(范围为 0 至 1;得分越高表示衰弱程度越高)。每日由专家临床医生访谈测量新发谵妄。
共有 247 名患者入院,218 名符合纳入/排除标准,平均年龄为 71.54 岁(标准差=9.53 岁),主要为白人(92.7%)和男性(91.7%)。参与者使用 FI 范围分组为非衰弱(FI<0.25,n=56(26%))、衰弱前期(FI=0.25-0.35,n=86(39%))和衰弱(FI>0.35,n=76(35%))。衰弱前期和衰弱与新发谵妄(非衰弱:3.6%vs衰弱前期:20.9%vs衰弱:29.3%,=0.001)和总谵妄天数(平均天数=非衰弱 0.04 vs衰弱前期 0.35 vs衰弱 0.57,=0.003)相关。在调整了社会人口因素后,衰弱前期(调整后的 OR=5.64,95%CI:1.23,25.99)和衰弱状态(调整后的 OR=6.80,95%CI:1.38,33.45)与谵妄独立相关。
本研究表明,衰弱指数与谵妄的发生独立相关,表明入院评估衰弱可能会识别出发生谵妄风险较高的患者。