Karakuchi Nozomi, Yanagawa Senichiro, Takei Daisuke, Kodama Shinya, Takeshima Yukio, Sumimoto Kazuo
Department of Surgery, Yoshida General Hospital, Akitakata City, Japan.
Department of Pathology, Graduate School of Biomedical and Health Sciences, Hiroshima University, Hiroshima, Japan.
Case Rep Oncol. 2020 Sep 28;13(3):1164-1170. doi: 10.1159/000510406. eCollection 2020 Sep-Dec.
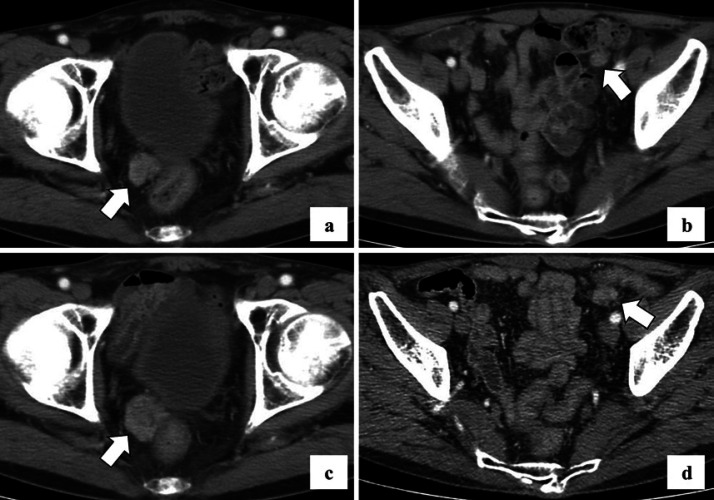
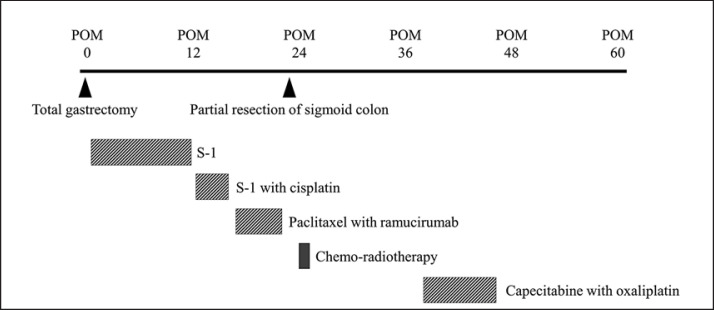
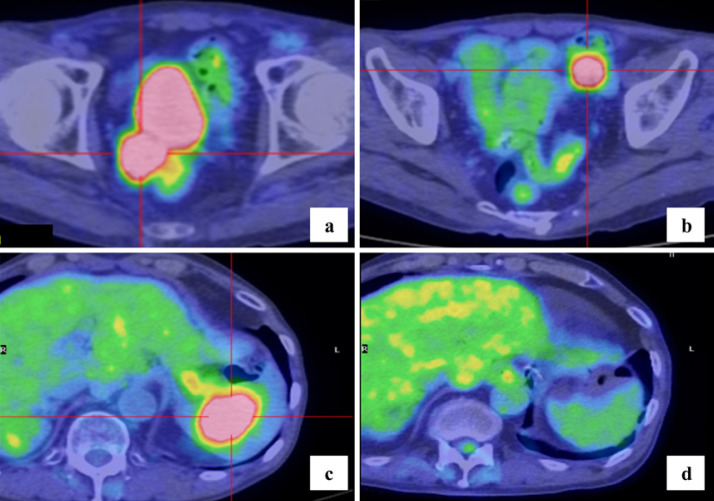
Splenic metastasis is known to occur at the terminal stage of cancer. While peritoneal dissemination is the most frequent recurrence of gastric cancer, metastasis to the spleen from gastric cancer is very rare. Splenectomy is currently the most effective probable treatment for solitary splenic metastasis of gastric cancer; it provides a good patient prognosis. However, careful consideration of surgical indications is required, as splenic metastasis is typically accompanied by multi-organ metastasis and dissemination. One of the main cancer treatment methods is the "wait-and-see" approach using chemotherapy. In general, patients with gastric cancer are treated with systemic chemotherapy for distant metastases including peritoneal dissemination. Radiotherapy is not commonly used to prolong life in patients with gastric cancer as gastric cancer is predominantly adenocarcinoma. However, a recent report indicated that chemo-radiotherapy was performed successfully for unresectable gastric cancer, including peritoneal dissemination. Here, we present the case of a 67-year-old patient who was observed to have peritoneal dissemination and splenic metastasis after gastric cancer surgery. Once the peritoneal dissemination was localized, surgical excision and chemo-radiotherapy were performed. We treated the splenic metastasis with the "wait-and-see" strategy with chemotherapy. A complete response on imaging in accordance with the Response Evaluation Criteria in Solid Tumors was achieved using multidisciplinary treatment. Our strategy of intensive multidisciplinary therapy could be a treatment option for cases with peritoneal dissemination or splenic metastasis of gastric cancer.
脾转移已知发生于癌症晚期。虽然腹膜播散是胃癌最常见的复发形式,但胃癌转移至脾脏非常罕见。脾切除术目前是治疗胃癌孤立性脾转移最有效的可能方法;它能为患者带来良好的预后。然而,由于脾转移通常伴有多器官转移和播散,所以需要仔细考虑手术指征。主要的癌症治疗方法之一是采用化疗的“观察等待”方法。一般来说,胃癌患者会接受全身化疗以治疗包括腹膜播散在内的远处转移。由于胃癌主要是腺癌,放疗在延长胃癌患者生命方面并不常用。然而,最近一份报告表明,化疗放疗已成功应用于无法切除的胃癌,包括腹膜播散。在此,我们报告一例67岁患者,其在胃癌手术后出现腹膜播散和脾转移。一旦腹膜播散局限化,便进行了手术切除和化疗放疗。我们采用化疗的“观察等待”策略治疗脾转移。根据实体瘤疗效评价标准,通过多学科治疗在影像学上实现了完全缓解。我们的强化多学科治疗策略可能是治疗胃癌腹膜播散或脾转移病例的一种选择。