Department of Hematology, Oncology, Clinical Immunology and Rheumatology, University Hospital Tübingen, Tübingen, Germany.
Department of Clinical Biochemistry and Immunology, Addenbrookes Hospital, Cambridge, UK.
BMC Infect Dis. 2020 Nov 11;20(1):828. doi: 10.1186/s12879-020-05553-y.
Severe and disseminated non-tuberculous mycobacterial (NTM) infections are frequently linked to a genetic predisposition but acquired defects of the interferon gamma (IFNγ) / interleukin 12 (IL-12) pathway need to be considered in adult patients with persistent or recurrent infections. Neutralizing anti-IFNγ autoantibodies disrupting IFNγ signalling have been identified as the cause of a severe and unique acquired immunodeficiency syndrome with increased susceptibility to NTM and other intracellular pathogens.
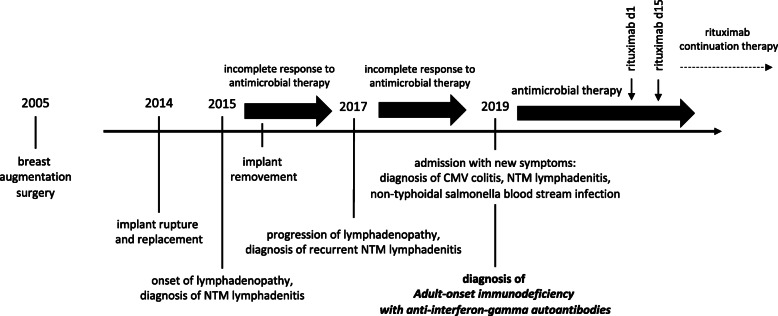
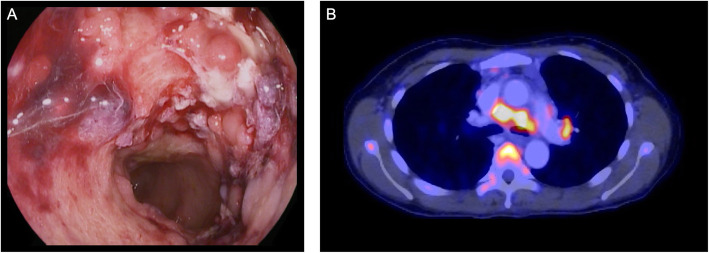
An adult Asian female with a previous history of recurrent NTM infections presented with persistent diarrhea, abdominal pain, night sweats and weight loss. Severe colitis due to a simultaneous infection with cytomegalovirus (CMV) and Salmonella typhimurium was diagnosed, with both pathogens also detectable in blood samples. Imaging studies further revealed thoracic as well as abdominal lymphadenopathy and a disseminated Mycobacterium intracellulare infection was diagnosed after a lymph node biopsy. Further diagnostics revealed the presence of high-titer neutralizing anti-IFNγ autoantibodies, allowing for the diagnosis of adult-onset immunodeficiency with anti-IFNγ autoantibodies (AIIA).
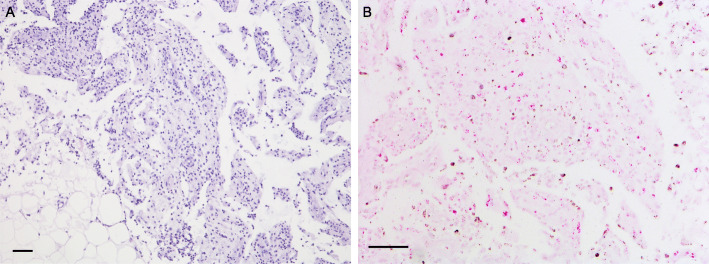
We here present a severe case of acquired immunodeficiency with anti-IFNγ autoantibodies with simultaneous, disseminated infections with both viral and microbial pathogens. The case illustrates how the diagnosis can cause considerable difficulties and is often delayed due to unusual presentations. Histological studies in our patient give further insight into the pathophysiological significance of impaired IFNγ signalling. B-cell-depleting therapy with rituximab offers a targeted treatment approach in AIIA.
严重且播散性非结核分枝杆菌(NTM)感染常与遗传易感性相关,但在持续性或复发性感染的成年患者中,需要考虑干扰素 γ(IFNγ)/白细胞介素 12(IL-12)通路获得性缺陷。已鉴定出中和抗 IFNγ 自身抗体破坏 IFNγ 信号传导,是导致严重且独特的获得性免疫缺陷综合征的原因,该综合征使 NTM 和其他细胞内病原体的易感性增加。
一名有复发性 NTM 感染既往史的成年亚裔女性,出现持续性腹泻、腹痛、盗汗和体重减轻。诊断为同时感染巨细胞病毒(CMV)和鼠伤寒沙门氏菌引起的严重结肠炎,血液样本中也可检测到这两种病原体。影像学研究进一步显示胸腹部淋巴结病,且淋巴结活检后诊断为播散性胞内分枝杆菌感染。进一步的诊断检查显示存在高滴度中和抗 IFNγ 自身抗体,从而诊断为成人发病的抗 IFNγ 自身抗体(AIIA)相关免疫缺陷。
我们在此介绍一例严重的 AIIA 合并同时播散性病毒和微生物病原体感染的获得性免疫缺陷病例。该病例说明了诊断可能会带来相当大的困难,且由于表现不典型,诊断往往会延迟。我们患者的组织学研究进一步深入了解了 IFNγ 信号传导受损的病理生理意义。利妥昔单抗的 B 细胞耗竭疗法为 AIIA 提供了一种靶向治疗方法。