NUTRIM School of Nutrition and Translational Research in Metabolism, Department of Health Promotion, Maastricht University, Maastricht, the Netherlands.
Independant Scholar, Kampala, Uganda.
BMC Pregnancy Childbirth. 2020 Nov 11;20(1):686. doi: 10.1186/s12884-020-03385-x.
The current maternal mortality ratio in Uganda is 336 maternal deaths per 100,000 live births. Infant mortality is 43 deaths per 1000 live births, with 42% of the mortality occurring during the neonatal period. This might be related to a weak health system in the country. This study aimed at assessing the uptake of lifesaving services during pregnancy and childbirth in Hoima District, Uganda.
The study used a cross-sectional quantitative design among 691 women with a child under 5 years. Households were randomly sampled from a list of all the villages in the district with the ENA for SMART software using the EPI methodology. Pre-coded questionnaires uploaded in the Open Data Kit were used for data collection. The data was cleaned and analysed using MS Excel and SPSS software. Descriptive results are presented.
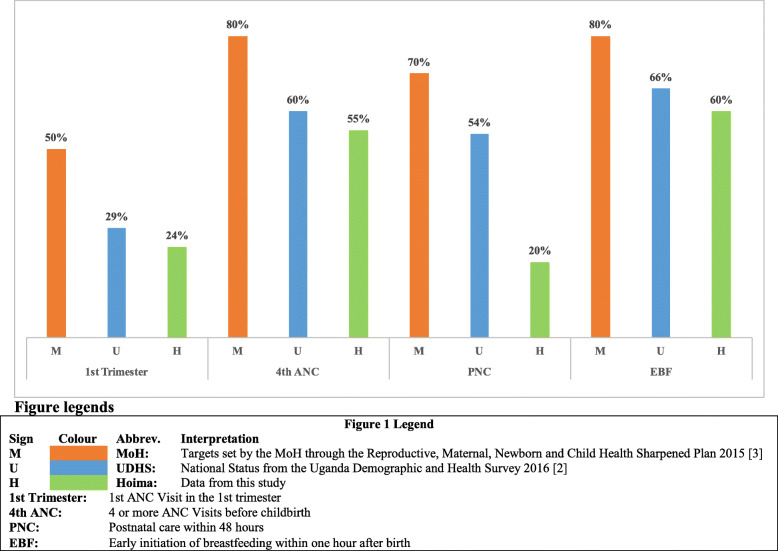
Of the 55.1% women attending at least four antenatal care (ANC) visits, only 24.3% had the first ANC within the first trimester. Moreover, ANC services generally was of poor quality, with only 0.4% meeting all the requirements for quality of ANC service. The highest contributors to this poor quality included poor uptake of iron-folic acid (adherence 28.8%), the six-required birth preparedness and complication readiness items (13.2%), and recognition of the seven danger signs of pregnancy (3.0%). Adherence to the seven essential newborn care actions was very low (0.5%), mainly caused by three practices: initiating breastfeeding within 1 h (59.9%), lack of postnatal care within 24 h (20.1%), and failure to recognize the 6 danger signs of the newborn (2.4%). Only 11.1% of the males participated in all maternal and newborn care requirements, by encouraging women to seek healthcare (39.9%), accompanying them to healthcare (36.9%), and HIV counselling and support services (26.2%).
The study reveals poor maternal and newborn practices throughout the continuum of care, from ANC and skilled birth attendance to newborn care during childbirth. With such poor results, it is not surprising that Hoima is sixth of 10 districts that have the highest numbers of deaths due to maternal mortality in Uganda.
乌干达目前的孕产妇死亡率为每 10 万例活产 336 例死亡。婴儿死亡率为每 1000 例活产死亡 43 例,其中 42%的死亡发生在新生儿期。这可能与该国薄弱的卫生系统有关。本研究旨在评估乌干达霍伊马区在妊娠和分娩期间接受拯救生命服务的情况。
该研究采用横断面定量设计,在 691 名 5 岁以下儿童的妇女中进行。使用 ENA for SMART 软件和 EPI 方法,根据该地区所有村庄的名单,对家庭进行随机抽样。使用预编码的问卷在 Open Data Kit 中进行数据收集。使用 MS Excel 和 SPSS 软件对数据进行清理和分析。呈现描述性结果。
在至少接受 4 次产前护理(ANC)就诊的 55.1%的妇女中,只有 24.3%的妇女在孕早期接受首次 ANC。此外,ANC 服务的质量普遍较差,仅有 0.4%符合 ANC 服务质量的所有要求。导致这种低质量的主要原因包括铁叶酸的低吸收率(遵医嘱率 28.8%)、6 项生育准备和并发症准备项目(13.2%)以及对 7 项妊娠危险征象的识别(3.0%)。对新生儿 7 项基本护理措施的遵医嘱率非常低(0.5%),主要原因是以下三项措施:在 1 小时内开始母乳喂养(59.9%)、产后 24 小时内未进行护理(20.1%)以及未能识别新生儿的 6 项危险征象(2.4%)。仅有 11.1%的男性参与了所有母婴保健要求,通过鼓励妇女寻求医疗保健(39.9%)、陪同她们去医疗保健(36.9%)以及艾滋病毒咨询和支持服务(26.2%)。
该研究表明,从 ANC 和熟练分娩护理到分娩期间的新生儿护理,整个母婴保健服务连续体的母婴保健实践都很差。由于这些结果很差,霍伊马区成为乌干达因产妇死亡率而导致死亡人数最多的 10 个区中的第六个区也就不足为奇了。