Kananura Rornald Muhumuza, Wamala Robert, Ekirapa-Kiracho Elizabeth, Tetui Moses, Kiwanuka Suzanne N, Waiswa Peter, Atuhaire Leonard K
Makerere University School of Public Health (MakSPH), Makerere University College of Health Sciences, Kampala, Uganda.
Department of Planning and Applied Statistics, Makerere University School of Statistics and Planning, Kampala, Uganda.
BMC Pregnancy Childbirth. 2017 Mar 27;17(1):98. doi: 10.1186/s12884-017-1289-5.
Neonatal and maternal health services have a bearing on neonatal mortality. Direct and indirect factors affecting neonatal health outcomes therefore require understanding to enable well-targeted interventions. This study, therefore, assessed the interrelationship between newborn health outcomes and maternal service utilization factors.
We investigated maternal health utilization factors using health facility delivery and at least four Antenatal Care (ANC) visits; and newborn health outcomes using newborn death and low birth weight (LBW). We used data from a household cross-sectional survey that was conducted in 2015 in Kamuli, Pallisa and Kibuku districts. We interviewed 1946 women who had delivered in the last 12 months. The four interrelated (Endogenous) outcomes were ANC attendance, health facility delivery, newborn death, and LBW. We performed analysis using a structural equation modeling technique.
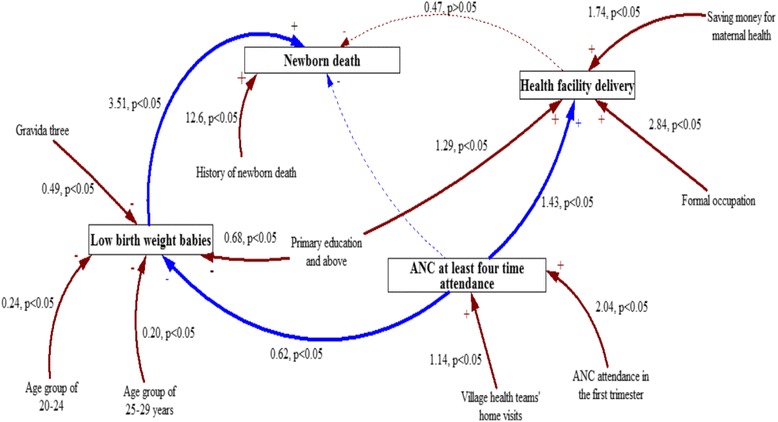
A history of newborn death (aOR = 12.64, 95% CI 5.31-30.10) and birth of a LBW baby (aOR = 3.51, 95% CI 1.48-8.37) were directly related to increased odds of newborn death. Factors that reduced the odds of LBW as a mediating factor for newborn death were ANC fourth time attendance (aOR = 0.62, 95% CI 0.45-0.85), having post-primary level education (aOR = 0.68, 95% CI 0.46-0.98) compared to none and being gravida three (aOR = 0.49, 95% CI 0.26-0.94) compared to being gravida one. Mother's age group, 20-24 (aOR = 0.24, 95% CI 0.08-0.75) and 25-29 years (aOR = 0.20, 95% CI 0.05-0.86) compared to 15-19 years was also associated with reduced odds of LBW. Additionally, ANC visits during the first trimester (aOR = 2.04, 95% CI 1.79-2.34), and village health teams (VHTs) visits while pregnant (aOR = 1.14, 95% CI 1.01-1.30) were associated with increased odds of at least four ANC visits, which is a mediating factor for health facility delivery, LBW and newborn death. Surprisingly, newborn death was not significantly different between health facility and community deliveries.
Attending ANC at least four times was a mediating factor for reduced newborn death and low birth weight. Interventions in maternal health and newborn health should focus on factors that increase ANC fourth time attendance and those that reduce LBW especially in resource-limited settings. Targeting women with high-risk pregnancies is also crucial for reducing newborn deaths.
新生儿和孕产妇健康服务与新生儿死亡率相关。因此,需要了解影响新生儿健康结局的直接和间接因素,以便进行有针对性的干预。因此,本研究评估了新生儿健康结局与孕产妇服务利用因素之间的相互关系。
我们通过医疗机构分娩和至少四次产前检查(ANC)来调查孕产妇健康利用因素;通过新生儿死亡和低出生体重(LBW)来调查新生儿健康结局。我们使用了2015年在卡穆利、帕利萨和基布库地区进行的一项家庭横断面调查的数据。我们采访了1946名在过去12个月内分娩的妇女。四个相互关联(内生)的结局是ANC就诊、医疗机构分娩、新生儿死亡和低出生体重。我们使用结构方程建模技术进行分析。
新生儿死亡史(调整后比值比[aOR]=12.64,95%置信区间[CI]5.31-30.10)和低出生体重儿出生(aOR=3.51,95%CI 1.48-8.37)与新生儿死亡几率增加直接相关。作为新生儿死亡中介因素,降低低出生体重几率的因素包括第四次ANC就诊(aOR=0.62,95%CI 0.45-0.85)、与未接受教育相比接受小学后教育(aOR=0.68,95%CI 0.46-0.98)以及与初产妇相比经产妇(aOR=0.49,95%CI 0.26-0.94)。母亲年龄组,与15-19岁相比,20-24岁(aOR=0.24,95%CI 0.08-0.75)和25-29岁(aOR=0.20,95%CI 从0.05-0.86)也与低出生体重几率降低相关。此外,孕早期的ANC就诊(aOR=2.04,95%CI 1.79-2.34)以及孕期村卫生室(VHT)就诊(aOR=1.14,95%CI 1.01-1.30)与至少四次ANC就诊几率增加相关,而这是医疗机构分娩、低出生体重和新生儿死亡的中介因素。令人惊讶的是,医疗机构分娩和社区分娩的新生儿死亡没有显著差异。
至少四次参加ANC是降低新生儿死亡和低出生体重的中介因素。孕产妇健康和新生儿健康干预应侧重于增加第四次ANC就诊的因素以及降低低出生体重的因素,尤其是在资源有限的环境中。针对高危妊娠妇女对于降低新生儿死亡也至关重要。