Makam Anil N, Nguyen Oanh Kieu, Miller Michael E, Shah Sachin J, Kapinos Kandice A, Halm Ethan A
Department of Internal Medicine, UT Southwestern Medical Center, Dallas, TX, USA.
Department of Population and Data Sciences, UT Southwestern Medical Center, Dallas, TX, USA.
BMC Health Serv Res. 2020 Nov 11;20(1):1032. doi: 10.1186/s12913-020-05847-6.
Long-term acute care hospital (LTACH) use varies considerably across the U.S., which may reflect uncertainty about the effectiveness of LTACHs vs. skilled nursing facilities (SNF), the principal post-acute care alternative. Given that LTACHs provide more intensive care and thus receive over triple the reimbursement of SNFs for comparable diagnoses, we sought to compare outcomes and spending between LTACH versus SNF transfer.
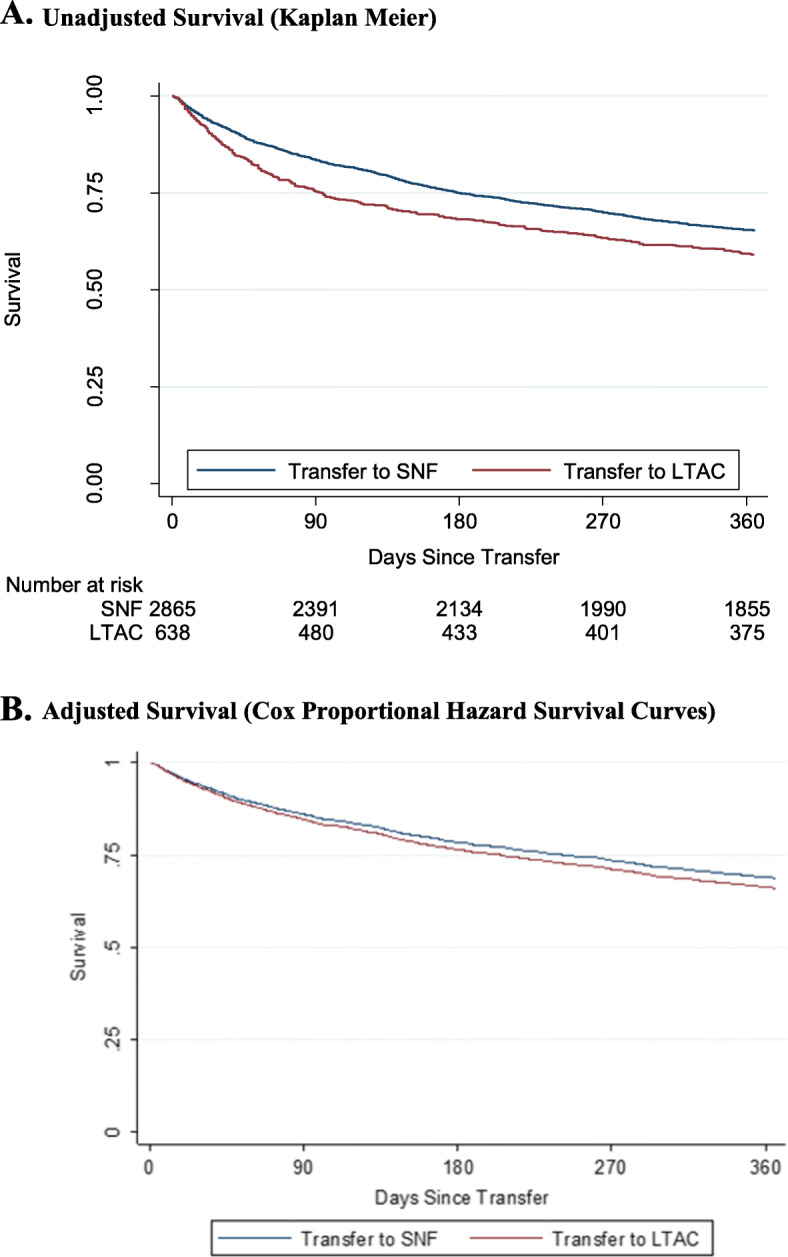
Using Medicare claims linked to electronic health record (EHR) data from six Texas Hospitals between 2009 and 2010, we conducted a retrospective cohort study of patients hospitalized on a medicine service in a high-LTACH use region and discharged to either an LTACH or SNF and followed for one year. The primary outcomes included mortality, 60-day recovery without inpatient care, days at home, and healthcare spending RESULTS: Of 3503 patients, 18% were transferred to an LTACH. Patients transferred to LTACHs were younger (median 71 vs. 82 years), less likely to be female (50.5 vs 66.6%) and white (69.0 vs. 84.1%), but were sicker (24.3 vs. 14.2% for prolonged intensive care unit stay; median diagnosis resource intensity weight of 2.03 vs. 1.38). In unadjusted analyses, patients transferred to an LTACH vs. SNF were less likely to survive (59.1 vs. 65.0%) or recover (62.5 vs 66.0%), and spent fewer days at home (186 vs. 200). Adjusting for demographic and clinical confounders available in Medicare claims and EHR data, LTACH transfer was not significantly associated with differences in mortality (HR, 1.12, 95% CI, 0.94-1.33), recovery (SHR, 1.07, 0.93-1.23), and days spent at home (IRR, 0.96, 0.83-1.10), but was associated with greater Medicare spending ($16,689 for one year, 95% CI, $12,216-$21,162).
LTACH transfer for Medicare beneficiaries is associated with similar clinical outcomes but with higher healthcare spending compared to SNF transfer. LTACH use should be reserved for patients who require complex inpatient care and cannot be cared for in SNFs.
长期急性病医院(LTACH)在美国各地的使用差异很大,这可能反映出与主要的急性后期护理替代机构——熟练护理设施(SNF)相比,LTACH有效性的不确定性。鉴于LTACH提供更强化的护理,因此对于可比诊断,其获得的报销是SNF的三倍多,我们试图比较LTACH与SNF转诊之间的结局和费用。
利用2009年至2010年期间与德克萨斯州六家医院的电子健康记录(EHR)数据相关联的医疗保险理赔数据,我们对在LTACH高使用地区因内科服务住院、出院后转至LTACH或SNF并随访一年的患者进行了一项回顾性队列研究。主要结局包括死亡率、无需住院护理的60天康复情况、在家天数以及医疗保健费用。结果:在3503名患者中,18%被转至LTACH。转至LTACH的患者更年轻(中位数分别为71岁和82岁),女性比例更低(分别为50.5%和66.6%),白人比例更低(分别为69.0%和84.1%),但病情更严重(长时间入住重症监护病房的比例分别为24.3%和14.2%;诊断资源强度权重中位数分别为2.03和1.38)。在未调整分析中,转至LTACH的患者与转至SNF的患者相比,存活可能性更低(分别为59.1%和65.0%)或康复可能性更低(分别为62.5%和66.0%),在家天数更少(分别为186天和200天)。在对医疗保险理赔数据和EHR数据中可用的人口统计学和临床混杂因素进行调整后,LTACH转诊与死亡率差异(风险比[HR],1.12,95%置信区间[CI],0.94 - 1.33)、康复差异(标准化风险比[SHR],1.07,0.93 - 1.23)以及在家天数差异(发病率比值比[IRR],0.96,0.83 - 1.10)无显著关联,但与更高的医疗保险费用相关(一年为16,689美元,95% CI,12,216 - 21,162美元)。
与SNF转诊相比,医疗保险受益人的LTACH转诊临床结局相似,但医疗保健费用更高。LTACH的使用应仅限于需要复杂住院护理且无法在SNF接受护理的患者。