Division of Cardiovascular Diseases, Department of Internal Medicine, University of Iowa Hospitals and Clinics, Iowa City.
Heart and Vascular Institute, Cleveland Clinic, Cleveland, Ohio.
JAMA Netw Open. 2020 Nov 2;3(11):e2025118. doi: 10.1001/jamanetworkopen.2020.25118.
Information regarding the performance and outcomes of noncardiac surgery (NCS) in patients with left ventricular assist devices (LVADs) is scarce, with limited longitudinal follow-up data that are mostly limited to single-center reports.
To examine the trends, patient characteristics, and outcomes associated with NCS among patients with LVAD.
DESIGN, SETTING, AND PARTICIPANTS: This cohort study examined patients enrolled in Medicare undergoing durable LVAD implantation from January 2012 to November 2017 with follow-up through December 2017. The study included all Medicare Provider and Analysis Review Part A files for the years 2012 to 2017. Patients identified by International Classification of Diseases, Ninth Revision Clinical Modification (ICD-9-CM) and International Classification of Diseases, Tenth Revision (ICD-10) procedure codes for new LVAD implantation were included. Data analysis was performed from November 2019 to February 2020.
NCS procedures were identified using the ICD-9-CM and ICD-10 procedural codes and divided into elective and urgent or emergent.
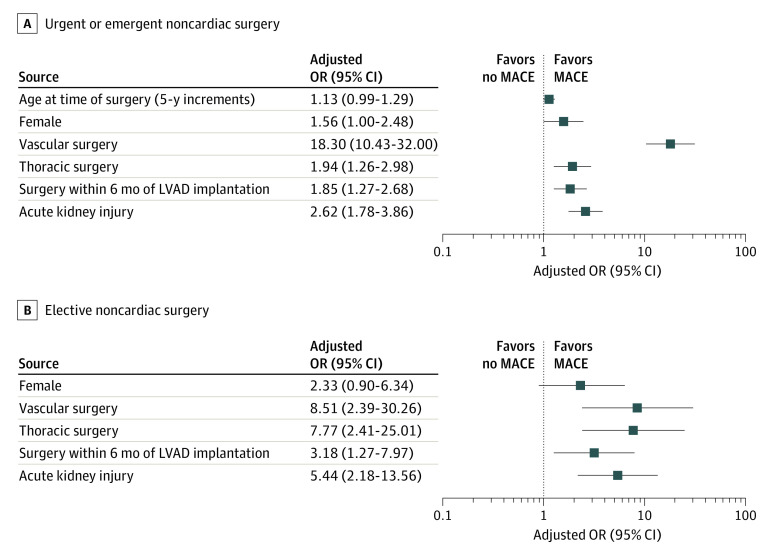
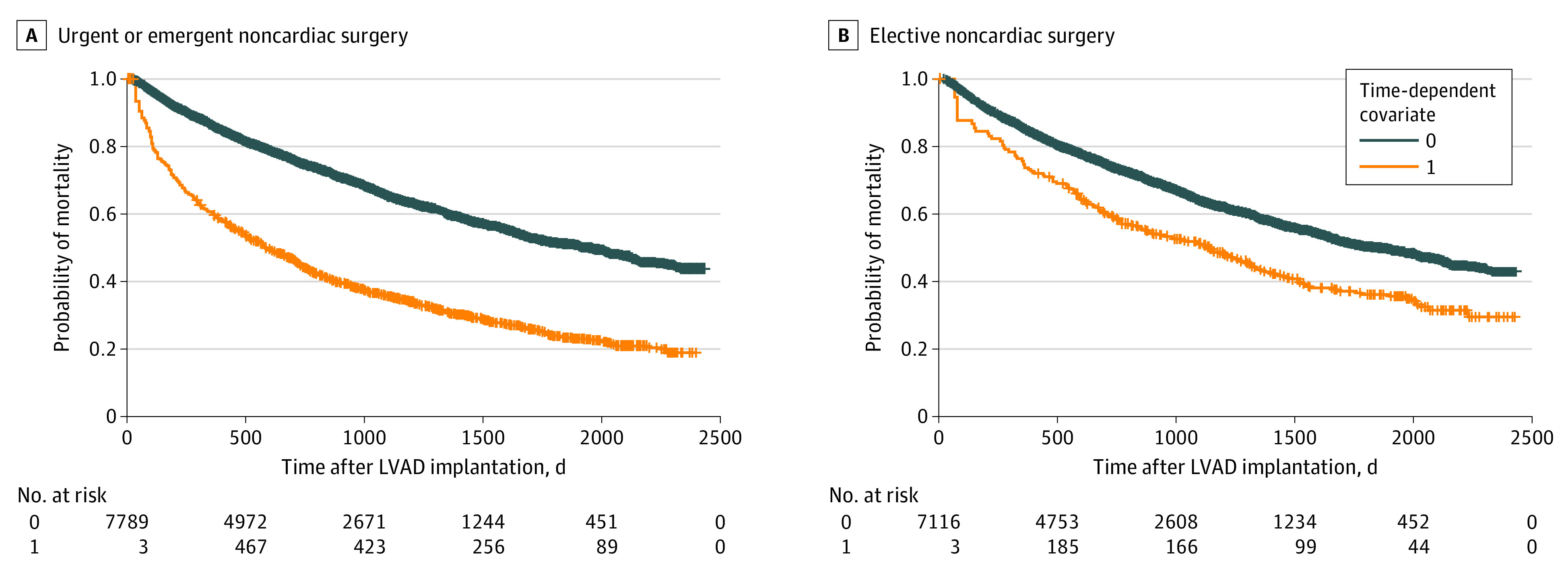
The primary outcome was major adverse cardiovascular events (MACEs), defined as in-hospital or 30-day all-cause mortality, ischemic stroke, or intracerebral hemorrhage after NCS. Early (<60 days after NCS) and late (≥60 days after NCS) mortality after NCS were analyzed in both subgroups using time-varying covariate and landmark analysis using patients who did not undergo NCS as reference.
Of the 8118 patients with LVAD (mean [SD] age, 63.4 [10.8] years; 6484 men [79.9%]), 1326 (16.3%, or approximately 1 in 6) underwent NCS, of which 1000 procedures (75.4%) were emergent or urgent and 326 (24.6%) were elective. There was no difference in age between patients who underwent NCS and patients who did not (mean [SD] age, 63.6 [10.6] vs 63.4 [10.9] years). The number of NCS procedures among patients with LVAD increased from 64 in 2012 to 304 in 2017. The median (interquartile range) time from LVAD implantation to NCS was 309 (133-606) days. The most frequent type of NCS was general (613 abdominal, pelvic, and gastrointestinal procedures [46.2%]). Perioperative MACEs occurred in 169 patients (16.9%) undergoing emergent or urgent NCS and 23 patients (7.1%) undergoing elective NCS. Urgent or emergent NCS was associated with higher mortality early (adjusted hazard ratio [aHR], 8.78; 95% CI, 7.20-10.72; P < .001) and late (aHR, 1.71; 95% CI, 1.53-1.90; P < .001) after NCS compared with patients with LVAD who did not undergo NCS. Elective NCS was also associated with higher mortality early (aHR, 2.65; 95% CI, 1.74-4.03; P < .001) and late (aHR, 1.29; 95% CI, 1.07-1.56; P = .008) after NCS.
One of 6 patients with LVAD underwent NCS. Perioperative MACEs were frequent. Higher mortality risk transcended the early postoperative period in urgent or emergent and elective surgical procedures.
关于左心室辅助装置 (LVAD) 患者非心脏手术 (NCS) 的表现和结果的信息很少,纵向随访数据有限,且主要限于单中心报告。
检查 LVAD 患者 NCS 的趋势、患者特征和结果。
设计、地点和参与者:这项队列研究检查了 2012 年 1 月至 2017 年 11 月期间接受耐用性 LVAD 植入的 Medicare 患者,并在 2017 年 12 月进行了随访。该研究包括 2012 年至 2017 年所有 Medicare 提供者和分析审查部分 A 文件。通过国际疾病分类第 9 修订版临床修改 (ICD-9-CM) 和国际疾病分类第 10 版 (ICD-10) 新 LVAD 植入程序代码确定患者。数据分析于 2019 年 11 月至 2020 年 2 月进行。
使用 ICD-9-CM 和 ICD-10 程序代码识别 NCS 程序,并分为选择性和紧急或紧急。
主要结果是主要心血管不良事件 (MACE),定义为 NCS 后住院或 30 天全因死亡率、缺血性中风或颅内出血。使用时间变化协变量和使用未接受 NCS 的患者作为参考的 landmark 分析分析了 NCS 后早期(NCS 后<60 天)和晚期(NCS 后≥60 天)死亡率。
在 8118 名 LVAD 患者(平均[标准差]年龄,63.4[10.8]岁;6484 名男性[79.9%])中,1326 名(16.3%,约 1 例中有 6 例)接受了 NCS,其中 1000 例(75.4%)为紧急或紧急手术,326 例(24.6%)为选择性手术。接受 NCS 和未接受 NCS 的患者之间的年龄无差异(平均[标准差]年龄,63.6[10.6]岁 vs 63.4[10.9]岁)。LVAD 植入后接受 NCS 的患者数量从 2012 年的 64 例增加到 2017 年的 304 例。LVAD 植入后接受 NCS 的中位数(四分位距)时间为 309(133-606)天。最常见的 NCS 类型是普外科(613 例腹部、盆腔和胃肠道手术[46.2%])。紧急或紧急 NCS 发生 169 例(16.9%),择期 NCS 发生 23 例(7.1%)。紧急或紧急 NCS 后早期(校正后的危险比[aHR],8.78;95%CI,7.20-10.72;P<0.001)和晚期(aHR,1.71;95%CI,1.53-1.90;P<0.001)死亡率高于未接受 NCS 的 LVAD 患者。选择性 NCS 后早期(aHR,2.65;95%CI,1.74-4.03;P<0.001)和晚期(aHR,1.29;95%CI,1.07-1.56;P=0.008)死亡率也高于未接受 NCS 的 LVAD 患者。
每 6 名 LVAD 患者中就有 1 名接受 NCS。围手术期 MACE 很常见。紧急或紧急手术和选择性手术的高死亡率风险超过了术后早期。