Kundi Harun, Valsdottir Linda R, Popma Jeffrey J, Cohen David J, Strom Jordan B, Pinto Duane S, Shen Changyu, Yeh Robert W
Richard A. and Susan F. Smith Center for Outcomes Research in Cardiology, Beth Israel Deaconess Medical Center, Boston, MA (H.K., L.R.V., J.J.P., J.B.S., D.S.P., C.S., R.W.Y.).
Saint Luke's Mid-America Heart Institute, Kansas City, MO (D.J.C.).
Circ Cardiovasc Qual Outcomes. 2018 Oct;11(10):e005048. doi: 10.1161/CIRCOUTCOMES.118.005048.
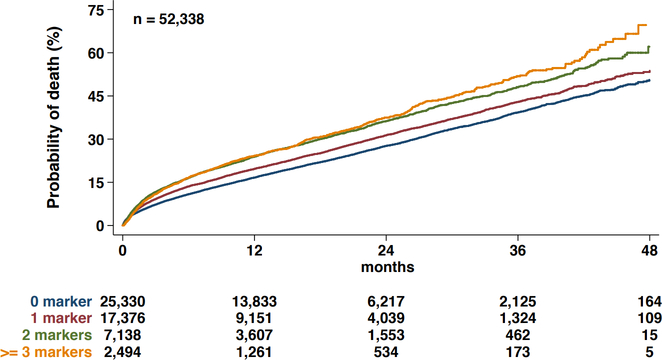
Background Prospectively collected frailty markers are associated with an incremental 1-year mortality risk after transcatheter aortic valve replacement (TAVR) compared with comorbidities alone. Whether information on frailty markers captured retrospectively in administrative billing data is similarly predictive of long-term mortality after TAVR is unknown. We sought to characterize the prognostic importance of frailty factors as identified in healthcare billing records in comparison to validated measures of frailty for the prediction of long-term mortality after TAVR. Methods and Results Adult patients undergoing TAVR between August 25, 2011, and September 29, 2015, were identified among Medicare fee-for-service beneficiaries. The Johns Hopkins Claims-based Frailty Indicator was used to identify frail patients. We used nested Cox regression models to identify claims-based predictors of mortality up to 4 years post-procedure. Four groups of variables, including cardiac risk factors, noncardiac risk factors, patient procedural risk factors, and nontraditional markers of frailty, were introduced sequentially, and their integrated discrimination improvement was assessed. A total of 52 338 TAVR patients from 558 clinical sites were identified, with a mean follow-up time period of 16 months. In total, 14 174 (27.1%) patients died within the study period. The mortality rate was 53.9% at 4 years post-TAVR. A total of 34 863 (66.6%) patients were defined as frail. The discrimination of each of the 4 models was 0.60 (95% CI, 0.59-60), 0.65 (95% CI, 0.64-0.65), 0.68 (95% CI, 0.67-0.68), and 0.70 (95% CI, 0.69-0.70), respectively. The addition of nontraditional frailty markers as identified in claims improved mortality prediction above and beyond traditional risk factors (integrated discrimination improvement: 0.019; P<0.001). Conclusions Risk prediction models that include frailty as identified in claims data can be used to predict long-term mortality risk after TAVR. Linkage to claims data may allow enhanced mortality risk prediction for studies that do not collect information on frailty.
背景 与仅考虑合并症相比,前瞻性收集的衰弱标志物与经导管主动脉瓣置换术(TAVR)后1年死亡风险的增加相关。在行政计费数据中回顾性获取的衰弱标志物信息是否同样能预测TAVR后的长期死亡率尚不清楚。我们试图通过与已验证的衰弱测量方法进行比较,来描述医疗计费记录中确定的衰弱因素对预测TAVR后长期死亡率的预后重要性。
方法与结果 在医疗保险按服务收费受益人中,确定了2011年8月25日至2015年9月29日期间接受TAVR的成年患者。使用基于约翰霍普金斯索赔的衰弱指标来识别衰弱患者。我们使用嵌套Cox回归模型来识别术后4年内基于索赔的死亡预测因素。依次引入四组变量,包括心脏危险因素、非心脏危险因素、患者手术危险因素和非传统衰弱标志物,并评估它们的综合判别改善情况。共识别出558个临床站点的52338例TAVR患者,平均随访时间为16个月。在研究期间,共有14174例(27.1%)患者死亡。TAVR术后4年的死亡率为53.9%。共有34863例(66.6%)患者被定义为衰弱。四个模型各自的判别度分别为0.60(95%CI,0.59 - 60)、0.65(95%CI,0.64 - 0.65)、0.68(95%CI,0.67 - 0.68)和0.70(95%CI,0.69 - 0.70)。与传统危险因素相比,索赔中确定的非传统衰弱标志物的加入改善了死亡率预测(综合判别改善:0.019;P<0.001)。
结论 包含索赔数据中确定的衰弱因素的风险预测模型可用于预测TAVR后的长期死亡风险。与索赔数据的关联可能有助于未收集衰弱信息的研究增强死亡风险预测。