Neonatal Medicine, School of Public Health, Faculty of Medicine, Imperial College London, London, UK.
NIHR Policy Research Unit in Maternal and Neonatal Health and Care, National Perinatal Epidemiology Unit, Nuffield Department of Population Health, University of Oxford, Oxford, UK.
Lancet Child Adolesc Health. 2021 Feb;5(2):113-121. doi: 10.1016/S2352-4642(20)30342-4. Epub 2020 Nov 9.
Babies differ from older children with regard to their exposure to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). However, data describing the effect of SARS-CoV-2 in this group are scarce, and guidance is variable. We aimed to describe the incidence, characteristics, transmission, and outcomes of SARS-CoV-2 infection in neonates who received inpatient hospital care in the UK.
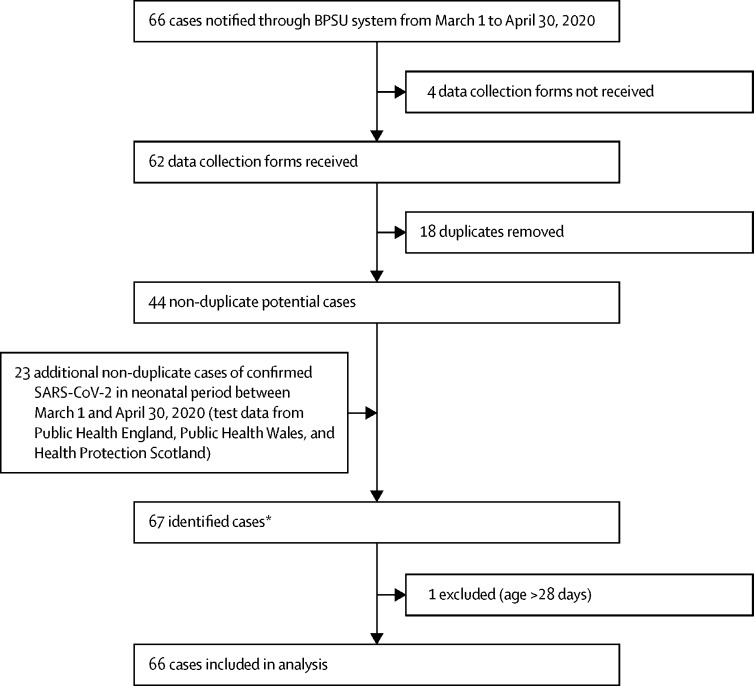
We carried out a prospective UK population-based cohort study of babies with confirmed SARS-CoV-2 infection in the first 28 days of life who received inpatient care between March 1 and April 30, 2020. Infected babies were identified through active national surveillance via the British Paediatric Surveillance Unit, with linkage to national testing, paediatric intensive care audit, and obstetric surveillance data. Outcomes included incidence (per 10 000 livebirths) of confirmed SARS-CoV-2 infection and severe disease, proportions of babies with suspected vertically and nosocomially acquired infection, and clinical outcomes.
We identified 66 babies with confirmed SARS-CoV-2 infection (incidence 5·6 [95% CI 4·3-7·1] per 10 000 livebirths), of whom 28 (42%) had severe neonatal SARS-CoV-2 infection (incidence 2·4 [1·6-3·4] per 10 000 livebirths). 16 (24%) of these babies were born preterm. 36 (55%) babies were from white ethnic groups (SARS-CoV-2 infection incidence 4·6 [3·2-6·4] per 10 000 livebirths), 14 (21%) were from Asian ethnic groups (15·2 [8·3-25·5] per 10 000 livebirths), eight (12%) were from Black ethnic groups (18·0 [7·8-35·5] per 10 000 livebirths), and seven (11%) were from mixed or other ethnic groups (5·6 [2·2-11·5] per 10 000 livebirths). 17 (26%) babies with confirmed infection were born to mothers with known perinatal SARS-CoV-2 infection, two (3%) were considered to have possible vertically acquired infection (SARS-CoV-2-positive sample within 12 h of birth where the mother was also positive). Eight (12%) babies had suspected nosocomially acquired infection. As of July 28, 2020, 58 (88%) babies had been discharged home, seven (11%) were still admitted, and one (2%) had died of a cause unrelated to SARS-CoV-2 infection.
Neonatal SARS-CoV-2 infection is uncommon in babies admitted to hospital. Infection with neonatal admission following birth to a mother with perinatal SARS-CoV-2 infection was unlikely, and possible vertical transmission rare, supporting international guidance to avoid separation of mother and baby. The high proportion of babies from Black, Asian, or minority ethnic groups requires investigation.
UK National Institute for Health Research Policy Research Programme.
婴儿与年长儿童相比,其接触严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)的情况有所不同。然而,描述该组中 SARS-CoV-2 影响的数据很少,并且指导意见也存在差异。我们旨在描述 2020 年 3 月 1 日至 4 月 30 日期间在英国住院的新生儿中 SARS-CoV-2 感染的发生率、特征、传播和结局。
我们进行了一项前瞻性英国基于人群的队列研究,纳入了在生命的头 28 天内确诊 SARS-CoV-2 感染且接受住院治疗的婴儿。通过英国儿科监测单位的主动国家监测发现感染婴儿,并与全国检测、儿科重症监护审核和产科监测数据相联系。结局包括确诊 SARS-CoV-2 感染和严重疾病的发生率(每 10000 例活产)、疑似垂直和医院内获得性感染婴儿的比例以及临床结局。
我们共发现 66 例确诊 SARS-CoV-2 感染的婴儿(发病率为 5.6[95%CI 4.3-7.1]每 10000 例活产),其中 28 例(42%)患有严重新生儿 SARS-CoV-2 感染(发病率为 2.4[1.6-3.4]每 10000 例活产)。16 例(24%)婴儿为早产儿。36 例(55%)婴儿来自白人种族群体(SARS-CoV-2 感染发病率为 4.6[3.2-6.4]每 10000 例活产),14 例(21%)来自亚洲种族群体(15.2[8.3-25.5]每 10000 例活产),8 例(12%)来自黑人种族群体(18.0[7.8-35.5]每 10000 例活产),7 例(11%)来自混合或其他种族群体(5.6[2.2-11.5]每 10000 例活产)。17 例确诊感染的婴儿出生于母亲围产期已知 SARS-CoV-2 感染的家庭,2 例(3%)被认为存在可能的垂直获得性感染(出生后 12 小时内的 SARS-CoV-2 阳性样本,而母亲也是阳性)。8 例(12%)婴儿存在疑似医院内获得性感染。截至 2020 年 7 月 28 日,58 例(88%)婴儿已出院回家,7 例(11%)仍在住院,1 例(2%)因与 SARS-CoV-2 感染无关的原因死亡。
新生儿 SARS-CoV-2 感染在住院婴儿中并不常见。出生后母亲围产期感染 SARS-CoV-2 而导致婴儿住院感染的可能性不大,可能的垂直传播也很少见,这支持了国际指南避免母婴分离的建议。来自黑人、亚洲或少数族裔群体的婴儿比例较高,需要进一步调查。
英国国家卫生研究院政策研究计划。