Department of Orthopaedics and Trauma, Hong Hui Hospital, Xi'an Jiaotong University College of Medicine, No. 555, East Youyi Road, Xi'an, 710000, Shaanxi, China.
Department of Orthopaedics and Trauma, The Second Affiliated Hospital of Xi'an Medical College, No. 167, East Textile Road, Xi'an, 710000, Shaanxi, China.
BMC Musculoskelet Disord. 2020 Nov 12;21(1):739. doi: 10.1186/s12891-020-03772-7.
Previous studies have demonstrated the effectiveness and safety of tranexamic acid (TXA) in orthopedic surgery. However, no study has investigated TXA in complex tibial plateau fracture surgery. Therefore, the purpose of this study was to confirm the safety and effectiveness of i.v. (intravenous) TXA and topical TXA.
This was a retrospective analysis of prospectively collected data. The control group received an equal amount of placebo (physiological saline solution); the i.v. group received 1.0 g TXA by intravenous injection before the tourniquet was inflated and before the surgical incision was closed, and the topical group received 3.0 g TXA in 75 mL of physiological saline solution 5 min prior to the final tourniquet release. Perioperative blood loss, vascular events, wound complications, and adverse reactions were compared among the three groups. The pain, knee function, and quality of life (QoL) assessments were based on their corresponding scoring systems.
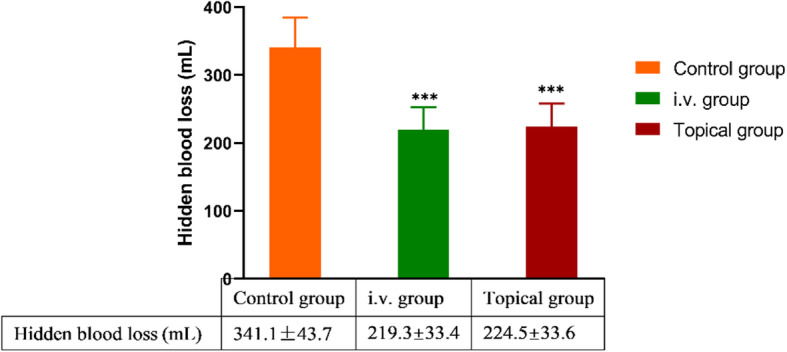
Baseline data were comparable for all groups. The i.v. group showed the best results for total blood loss (TBL) and hidden blood loss (HBL) (424.5 ± 49.4 mL and 219.3 ± 33.4 mL, respectively, all P values < 0.001). Patients in the i.v. group had lesser real Hb decrease than those in the control group (0.9 vs 1.5, P<0.001) and topical group (0.9 vs 1.2, P = 0.026). The blood coagulation level as measured using fibrinolysis (D-dimer) was lower in the i.v. group than in the control and topical groups on POD1 and POD3; however, this difference was not significant; the fibrin-degradation products also showed a similar trend. Patients in the topical group experienced less pain than those in the control group on POD2, POD4, and PO6W. The VAS pain score was 3.6 vs. 4.4 (POD2, P<0.05), 2.8 vs 3.3 (POD4, P<0.05), and 2.1 vs. 2.6 (PO6W, P<0.001) in the topical group vs control group, respectively. No significant differences were identified in vascular events, wound complications, adverse reactions, knee function, and QoL among the three groups.
To our knowledge, this is the first study that showed both i.v. TXA and topical TXA are safe and effective for complex tibial plateau fractures. The i.v. regimen effectively reduced blood loss during the perioperative period, whereas patients under the topical regimen had less vascular events, wound complications, and a lower incidence of adverse reactions compared to those in the i.v. group.
The trial was registered in the Chinese Clinical Trial Registry ( ChiCTR-TRC-1800017754 , retrospectively registered from 2018 to 01-01).
已有研究证实了氨甲环酸(TXA)在骨科手术中的有效性和安全性。但目前尚无研究探讨 TXA 在复杂胫骨平台骨折手术中的应用。因此,本研究旨在证实静脉注射 TXA 和局部 TXA 的安全性和有效性。
这是一项前瞻性数据的回顾性分析。对照组接受等量安慰剂(生理盐水);静脉组在止血带充气前和手术切口关闭前静脉注射 1.0g TXA,局部组在最后一次止血带释放前 5 分钟用 3.0g TXA 加 75ml 生理盐水。比较三组患者围手术期失血量、血管事件、伤口并发症和不良反应。疼痛、膝关节功能和生活质量(QoL)评估均基于相应的评分系统。
所有组的基线数据均具有可比性。静脉组总失血量(TBL)和隐性失血量(HBL)最佳(分别为 424.5±49.4ml 和 219.3±33.4ml,均 P<0.001)。与对照组和局部组相比,静脉组患者的实际 Hb 下降幅度较小(0.9 vs 1.5,P<0.001;0.9 vs 1.2,P=0.026)。第 1 天(POD1)和第 3 天(POD3),纤维蛋白溶解(D-二聚体)检测的凝血水平在静脉组低于对照组和局部组,但差异无统计学意义;纤维蛋白降解产物也呈现出类似的趋势。局部组患者在术后第 2 天(POD2)、第 4 天(POD4)和第 6 周(PO6W)时疼痛程度低于对照组。与对照组相比,局部组患者在术后第 2 天(POD2)时 VAS 疼痛评分(3.6 vs. 4.4,P<0.05)、第 4 天(POD4)时(2.8 vs. 3.3,P<0.05)和第 6 周(PO6W)时(2.1 vs. 2.6,P<0.001)疼痛评分较低。三组患者在血管事件、伤口并发症、不良反应、膝关节功能和 QoL 方面无显著差异。
据我们所知,这是第一项研究表明静脉 TXA 和局部 TXA 均安全有效治疗复杂胫骨平台骨折。静脉方案可有效减少围手术期失血,而局部方案与静脉组相比,血管事件、伤口并发症和不良反应发生率较低。
本研究在中国临床试验注册中心(ChiCTR-TRC-1800017754,从 2018 年 01-01 日开始回顾性注册)。