Institute of Applied Health Research, University of Birmingham, Birmingham, UK, and Warwick Medical School, University of Warwick, Coventry, UK.
Institute of Applied Health Research, University of Birmingham, Birmingham, UK.
Arthritis Rheumatol. 2021 May;73(5):731-739. doi: 10.1002/art.41593.
To identify whether active use of nonsteroidal antiinflammatory drugs (NSAIDs) increases susceptibility to developing suspected or confirmed coronavirus disease 2019 (COVID-19) compared to the use of other common analgesics.
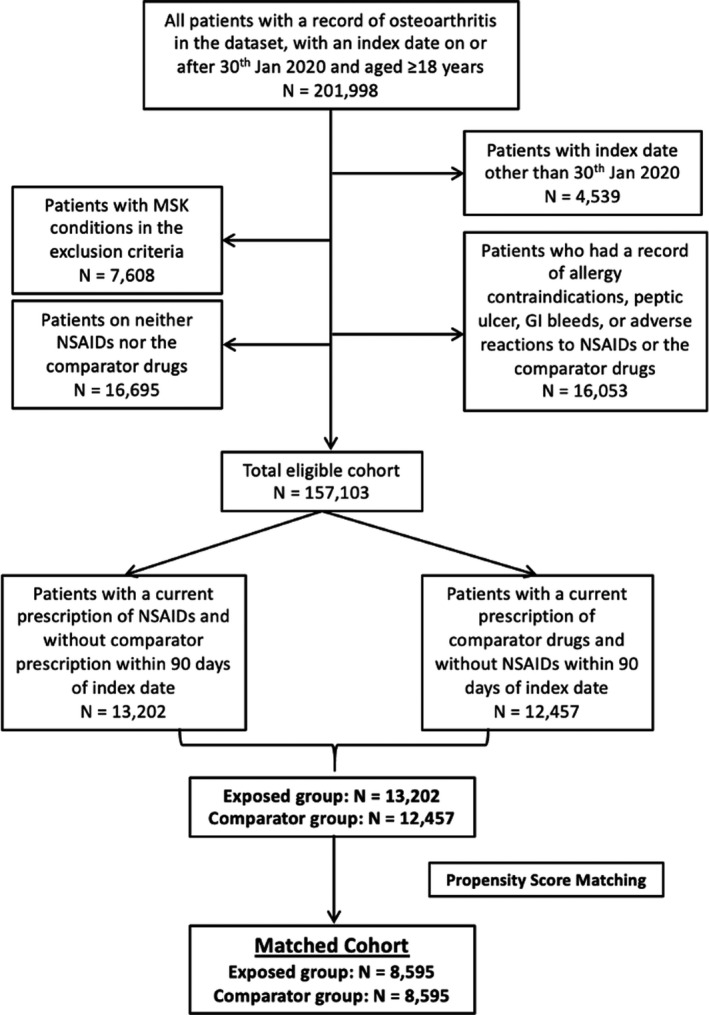
We performed a propensity score-matched cohort study with active comparators, using a large UK primary care data set. The cohort consisted of adult patients age ≥18 years with osteoarthritis (OA) who were followed up from January 30 to July 31, 2020. Patients prescribed an NSAID (excluding topical preparations) were compared to those prescribed either co-codamol (paracetamol and codeine) or co-dydramol (paracetamol and dihydrocodeine). A total of 13,202 patients prescribed NSAIDs were identified, compared to 12,457 patients prescribed the comparator drugs. The primary outcome measure was the documentation of suspected or confirmed COVID-19, and the secondary outcome measure was all-cause mortality.
During follow-up, the incidence rates of suspected/confirmed COVID-19 were 15.4 and 19.9 per 1,000 person-years in the NSAID-exposed group and comparator group, respectively. Adjusted hazard ratios for suspected or confirmed COVID-19 among the unmatched and propensity score-matched OA cohorts, using data from clinical consultations in primary care settings, were 0.82 (95% confidence interval [95% CI] 0.62-1.10) and 0.79 (95% CI 0.57-1.11), respectively, and adjusted hazard ratios for the risk of all-cause mortality were 0.97 (95% CI 0.75-1.27) and 0.85 (95% CI 0.61-1.20), respectively. There was no effect modification by age or sex.
No increase in the risk of suspected or confirmed COVID-19 or mortality was observed among patients with OA in a primary care setting who were prescribed NSAIDs as compared to those who received comparator drugs. These results are reassuring and suggest that in the absence of acute illness, NSAIDs can be safely prescribed during the ongoing pandemic.
与使用其他常见镇痛剂相比,确定积极使用非甾体抗炎药(NSAIDs)是否会增加罹患疑似或确诊 2019 年冠状病毒病(COVID-19)的易感性。
我们使用英国大型初级保健数据进行了倾向评分匹配的队列研究,并设置了活性对照。该队列包括年龄≥18 岁、患有骨关节炎(OA)的成年患者,随访时间为 2020 年 1 月 30 日至 7 月 31 日。将接受 NSAID(不包括局部制剂)治疗的患者与接受可待因复方片(对乙酰氨基酚和可待因)或双氢可待因片(对乙酰氨基酚和二氢可待因)治疗的患者进行比较。共确定了 13202 名接受 NSAID 治疗的患者,与 12457 名接受对照药物治疗的患者进行了比较。主要观察指标为疑似或确诊 COVID-19 的记录,次要观察指标为全因死亡率。
在随访期间,暴露于 NSAID 的患者和对照组患者的疑似/确诊 COVID-19 的发病率分别为每 1000 人年 15.4 和 19.9。在初级保健环境下的临床就诊中使用未匹配和倾向评分匹配的 OA 队列数据,疑似或确诊 COVID-19 的调整后的危险比分别为 0.82(95%置信区间[95%CI]为 0.62-1.10)和 0.79(95%CI 为 0.57-1.11),全因死亡率的调整后的危险比分别为 0.97(95%CI 为 0.75-1.27)和 0.85(95%CI 为 0.61-1.20)。年龄或性别均无影响修饰作用。
在初级保健环境中,与接受对照药物治疗的患者相比,OA 患者服用 NSAIDs 并未增加疑似或确诊 COVID-19 或死亡率的风险。这些结果令人放心,表明在没有急性疾病的情况下,在持续的大流行期间可以安全地开 NSAIDs。