Pharmaco- and Device Epidemiology, Centre for Statistics in Medicine-Nuffield Department of Orthopaedics, Rheumatology and Musculoskeletal Sciences, Botnar Research Centre, University of Oxford, Windmill Road, OX37LD, Oxford, UK.
IQVIA, Real World Solutions, Brighton, UK.
Drugs. 2023 Feb;83(3):249-263. doi: 10.1007/s40265-022-01822-z. Epub 2023 Jan 24.
We aimed to investigate whether ibuprofen use, compared with other non-selective non-steroidal anti-inflammatory drugs (ns-NSAIDs), cyclooxygenase-2 inhibitors (COX-2i) or paracetamol, increases the risk of coronavirus disease 2019 (COVID-19) diagnosis or hospitalisation.
A prevalent user and active comparator cohort study.
Two US claims databases (Open Claims and PharMetrics Plus) mapped to the Observational Medical Outcomes Partnership Common Data Model.
Insured patients with a history of osteoarthritis or back pain and receiving ibuprofen, other ns-NSAIDs, COX-2i or paracetamol between 1 November, 2019 and 31 January, 2020 (study enrolment window 1) or between 1 February, 2020 and 31 October, 2020 (study enrolment window 2).
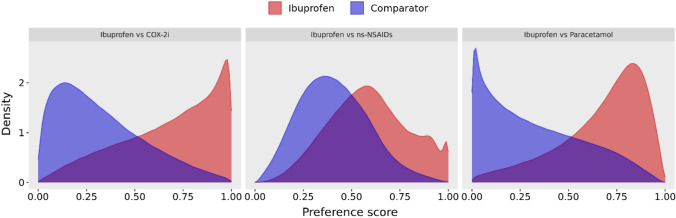
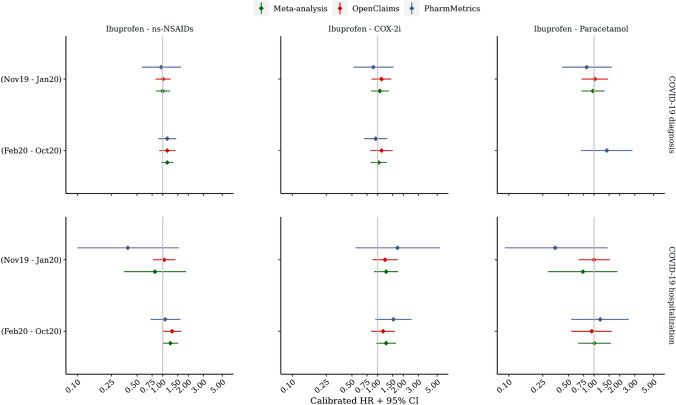
Large-scale propensity score matching and empirical calibration were used to minimise confounding. Incidence and hazard ratios of COVID-19 diagnosis and hospitalisation according to drug/s use were estimated and pooled in the same study period across data sources using a fixed-effects meta-analysis. Index treatment episode was the primary risk evaluation window, censored at the time of discontinuation.
A total of 633,562 and 1,063,960 participants were included in periods 1 and 2, respectively, for the ibuprofen versus ns-NSAIDs comparison, 311,669 and 524,470 for ibuprofen versus COX-2i, and 492,002 and 878,598 for ibuprofen versus paracetamol. Meta-analyses of empirically calibrated hazard ratios revealed no significantly differential risk of COVID-19 outcomes in users of ibuprofen versus any of the other studied analgesic classes: hazard ratios were 1.13 (0.96-1.33) for the ibuprofen-ns-NSAIDs comparison, 1.03 (0.83-1.28) for the ibuprofen-COX-2i comparison and 1.13 (0.74-1.73) for ibuprofen-paracetamol comparison on COVID-19 diagnosis in the February 2020-October 2020 window. Similar hazard ratios were found on COVID-19 hospitalisation and across both study periods.
In patients with osteoarthritis or back pain, we found no differential risks of incident COVID-19 diagnosis or COVID-19 hospitalisation for ibuprofen users compared with other ns-NSAIDs, COX-2i or paracetamol. Our findings support regulatory recommendations that NSAIDs, including ibuprofen, should be prescribed as indicated in the same way as before the COVID-19 pandemic, especially for those who rely on ibuprofen or NSAIDs to manage chronic arthritis or musculoskeletal pain symptoms.
我们旨在研究与其他非选择性非甾体抗炎药(ns-NSAIDs)、环氧化酶-2 抑制剂(COX-2i)或对乙酰氨基酚相比,布洛芬的使用是否会增加 2019 年冠状病毒病(COVID-19)诊断或住院的风险。
一项普遍使用者和活性对照队列研究。
两个美国索赔数据库(Open Claims 和 PharMetrics Plus)映射到观察性医疗结局伙伴关系通用数据模型。
2019 年 11 月 1 日至 2020 年 1 月 31 日(研究登记窗口 1)或 2020 年 2 月 1 日至 2020 年 10 月 31 日(研究登记窗口 2)期间,有骨关节炎或背痛病史且接受布洛芬、其他 ns-NSAIDs、COX-2i 或对乙酰氨基酚治疗的参保患者。
采用大规模倾向评分匹配和经验校准来最小化混杂因素。根据药物使用情况,估计 COVID-19 诊断和住院的发生率和风险比,并在同一研究期间使用固定效应荟萃分析在不同数据源中进行汇总。索引治疗期是主要的风险评估窗口,在停药时截止。
在第 1 期和第 2 期,分别有 633562 名和 1063960 名参与者纳入布洛芬与 ns-NSAIDs 比较组,311669 名和 524470 名参与者纳入布洛芬与 COX-2i 比较组,492002 名和 878598 名参与者纳入布洛芬与对乙酰氨基酚比较组。对经验校准风险比的荟萃分析显示,与其他研究的镇痛类药物相比,布洛芬使用者的 COVID-19 结局风险无显著差异:在 2020 年 2 月至 10 月窗口期,布洛芬与 ns-NSAIDs 比较的风险比为 1.13(0.96-1.33),布洛芬与 COX-2i 比较的风险比为 1.03(0.83-1.28),布洛芬与对乙酰氨基酚比较的风险比为 1.13(0.74-1.73)。在 COVID-19 住院方面也发现了类似的风险比,且横跨两个研究期。
在骨关节炎或背痛患者中,与其他 ns-NSAIDs、COX-2i 或对乙酰氨基酚相比,布洛芬使用者发生 COVID-19 诊断或 COVID-19 住院的风险无差异。我们的研究结果支持监管机构的建议,即在 COVID-19 大流行之前,应按照指示开处方使用 NSAIDs,包括布洛芬,特别是对于那些依赖布洛芬或 NSAIDs 来控制慢性关节炎或肌肉骨骼疼痛症状的患者。