Parasuraman Jaya Madhura, Kloprogge Frank, Standing Joseph Frank, Albur Mahableshwar, Heep Axel
Neonatal Intensive Care Unit, Southmead Hospital, Southmead Road, Bristol, United Kingdom, BS10 5NB; Infection, Inflammation and Rheumatology Section, Institute of Child Health, University College London, 30 Guilford Street, Holborn, London, United Kingdom, WC1N 1EH.
Institute for Global Health, University College London, 30 Guilford Street, Holborn, London, United Kingdom, WC1N 1EH.
Eur J Pharm Sci. 2021 Mar 1;158:105643. doi: 10.1016/j.ejps.2020.105643. Epub 2020 Nov 12.
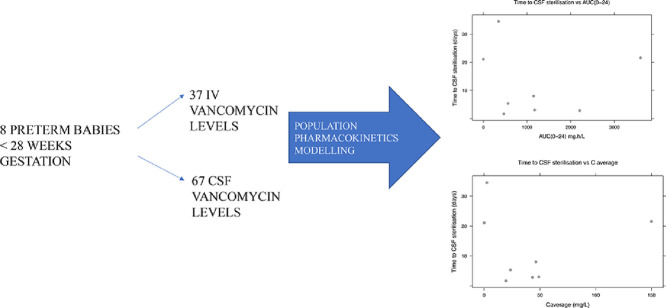
Intraventricular vancomycin is an effective treatment for neonatal ventriculitis, as the cerebrospinal fluid (CSF) vancomycin levels reach adequate concentrations to achieve microbiological cure. There is no robust data on intraventricular vancomycin pharmacokinetics in the preterm population. This pilot population pharmacokinetic modelling study examines the pharmacokinetic behaviour of intraventricular vancomycin in the preterm population of < 28 weeks gestation, to inform the feasibility of future prospective studies.
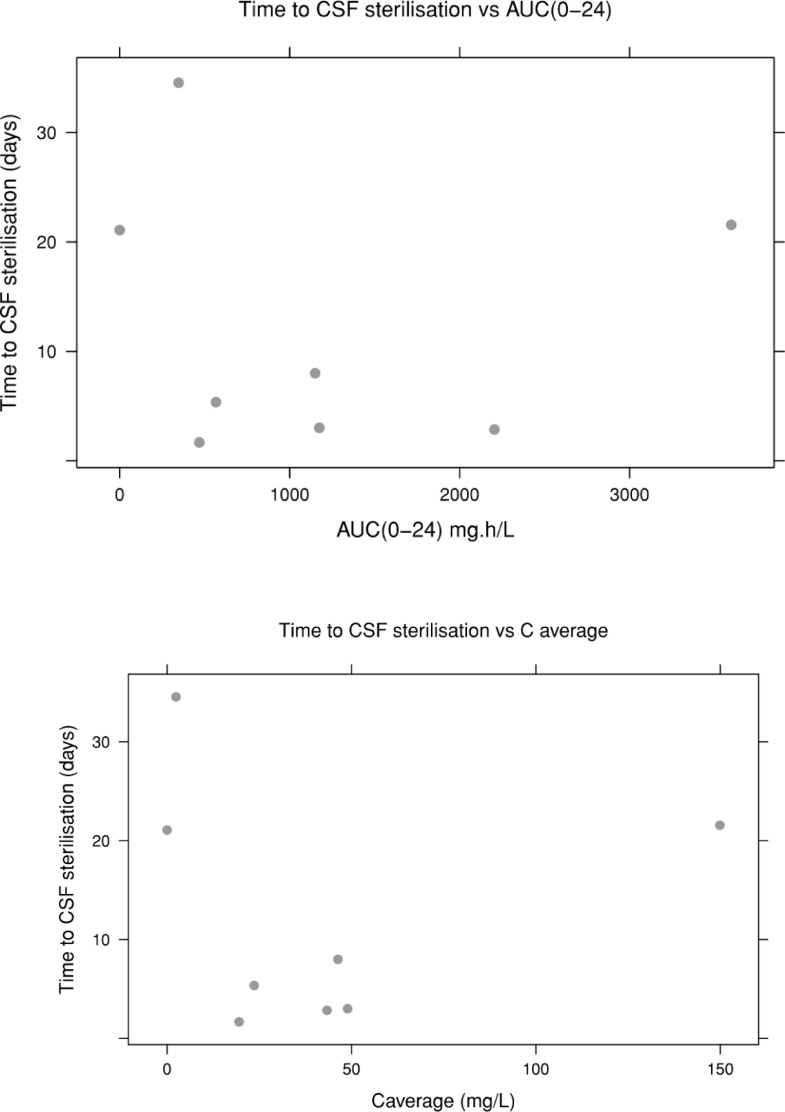
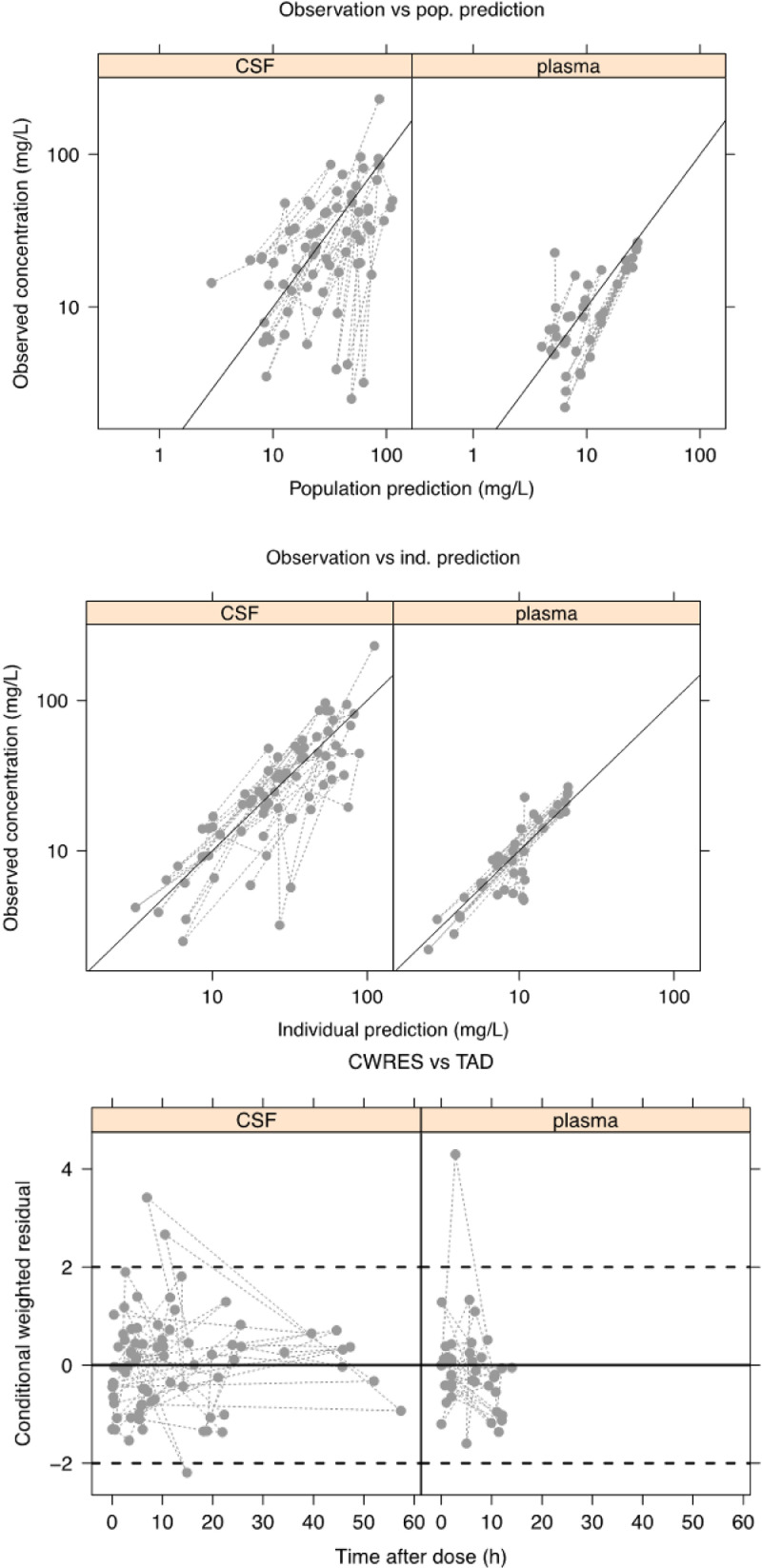
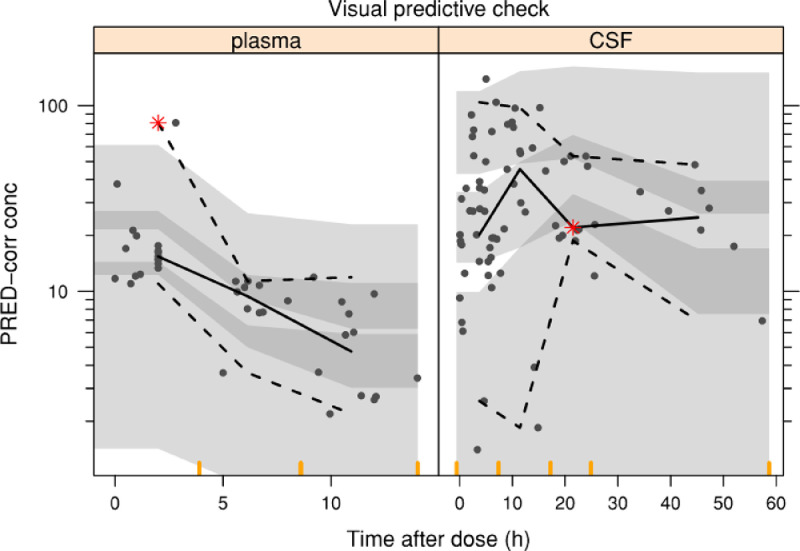
The study comprised 8 preterm infants with neonatal ventriculitis (median gestation age 25.3 weeks; range 23.9 - 27.7). Population pharmacokinetics (non-linear mixed effects modelling) were described with one- and two-compartment models to fit plasma concentrations of vancomycin. A CSF compartment was added to the plasma modelling and mass transfer examined. Three covariates (serum creatinine, ventricular index (VI) and CSF protein) were tested on the final model. Area under the curve (AUC) and average CSF concentration (C average) predictions were generated from the final model and compared with time to microbiological cure.
A one-compartment model provided the best fit to the data. There was no appreciable transfer between plasma and CSF. None of the covariates provided a significant reduction in the objective function value (OFV). Generally, time to sterilisation with higher CSF AUC (0-24) and C average tends to be shorter, however this should be interpreted with caution as data is erratic.
This pilot population pharmacokinetic analysis provides important information to warrant changes in the management of intraventricular vancomycin treatment in the preterm population, such as the current use of VI as a dosing parameter. Further study with a larger data pool is necessary to investigate the influence of VI on CSF vancomycin and ascertain dosing strategies.
脑室内注射万古霉素是治疗新生儿脑室炎的有效方法,因为脑脊液(CSF)中的万古霉素水平可达到足够浓度以实现微生物学治愈。关于早产儿脑室内注射万古霉素的药代动力学,目前尚无确凿数据。这项初步的群体药代动力学建模研究旨在探讨孕周小于28周的早产儿脑室内注射万古霉素的药代动力学行为,为未来前瞻性研究的可行性提供参考。
该研究纳入了8例患有新生儿脑室炎的早产儿(中位孕周25.3周;范围23.9 - 27.7周)。采用一室和二室模型描述群体药代动力学(非线性混合效应建模),以拟合万古霉素的血浆浓度。在血浆建模中增加了一个脑脊液室,并对物质传递进行了研究。在最终模型上测试了三个协变量(血清肌酐、脑室指数(VI)和脑脊液蛋白)。从最终模型生成曲线下面积(AUC)和脑脊液平均浓度(C平均)预测值,并与微生物学治愈时间进行比较。
一室模型对数据的拟合效果最佳。血浆和脑脊液之间没有明显的物质传递。没有一个协变量能使目标函数值(OFV)显著降低。一般来说,脑脊液AUC(0 - 24)和C平均较高时,杀菌时间往往较短,然而由于数据不稳定,对此应谨慎解释。
这项初步的群体药代动力学分析提供了重要信息,有必要改变早产儿脑室内注射万古霉素治疗的管理方式,比如目前将VI作为给药参数的做法。需要进一步用更大的数据集进行研究,以调查VI对脑脊液万古霉素的影响并确定给药策略。