Blassmann Ute, Roehr Anka C, Frey Otto R, Vetter-Kerkhoff Cornelia, Thon Niklas, Hope William, Briegel Josef, Huge Volker
Department of Pharmacy, University Hospital of Munich, Marchioninistrasse 15, Munich, 81377, Germany.
Department of Pharmacy, Heidenheim General Hospital, Schlosshausstrasse 100, Heidenheim, 89522, Germany.
Crit Care. 2016 Oct 24;20(1):343. doi: 10.1186/s13054-016-1523-y.
Ventriculitis is a complication of temporary intraventricular drains. The limited penetration of meropenem into the cerebrospinal fluid (CSF) is well known. However, ventricular CSF pharmacokinetic data in patients with ventriculitis are lacking. The aim of this study was to evaluate meropenem pharmacokinetics in the serum and CSF of neurocritical care patients with proven or suspected ventriculitis.
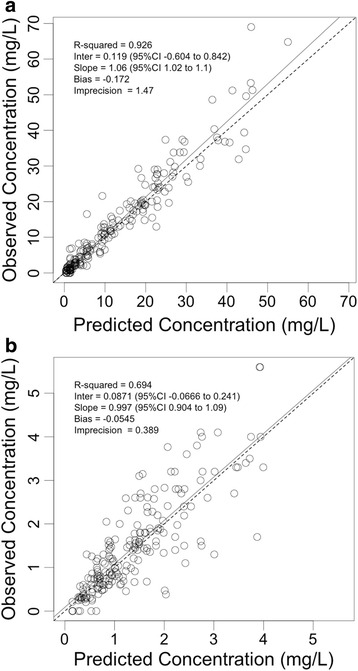
We conducted an observational pharmacokinetic study of neurocritical care patients with proven or suspected ventriculitis receiving meropenem. Multiple blood and CSF samples were taken and were described using nonparametric pharmacokinetic modelling with Pmetrics.
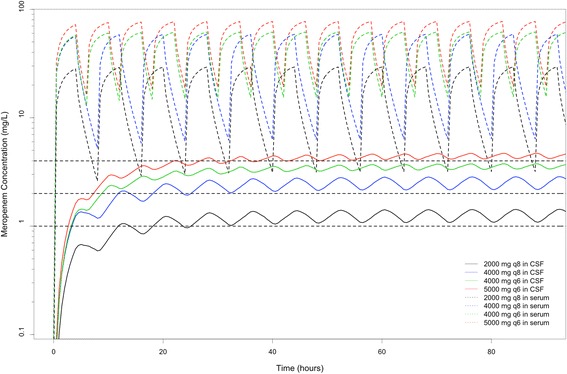
In total, 21 patients (median age 52 years, median weight 76 kg) were included. The median (range) of peak and trough concentrations in serum were 20.16 (4.40-69.00) mg/L and 2.54 (0.00-31.40) mg/L, respectively. The corresponding peak and trough concentrations in CSF were 1.20 (0.00-6.20) mg/L and 1.28 (0.00-4.10) mg/L, respectively, with a median CSF/serum ratio (range) of 0.09 (0.03-0.16). Median creatinine clearance ranged from 60.7 to 217.6 ml/minute (median 122.5 ml/minute). A three-compartment linear population pharmacokinetic model was most appropriate. No covariate relationships could be supported for any of the model parameters. Meropenem demonstrated poor penetration into CSF, with a median CSF/serum ratio of 9 % and high interindividual pharmacokinetic variability.
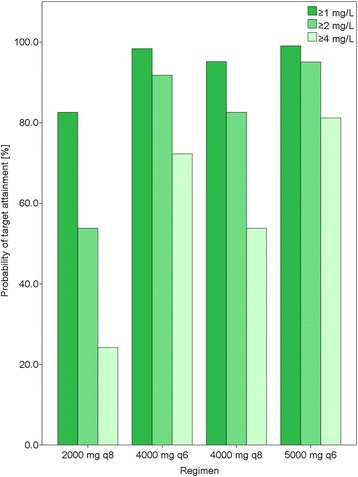
Administration of higher-than-standard doses of meropenem and therapeutic drug monitoring in both serum and CSF should be considered to individualise meropenem dosing in neurocritical care patients with ventriculitis.
脑室炎是临时性脑室内引流管的一种并发症。美罗培南在脑脊液(CSF)中的穿透性有限,这是众所周知的。然而,目前尚缺乏脑室炎患者的脑室CSF药代动力学数据。本研究的目的是评估确诊或疑似脑室炎的神经重症监护患者血清和CSF中美罗培南的药代动力学。
我们对确诊或疑似脑室炎且接受美罗培南治疗的神经重症监护患者进行了一项观察性药代动力学研究。采集了多份血液和CSF样本,并使用Pmetrics的非参数药代动力学模型进行描述。
共纳入21例患者(中位年龄52岁,中位体重76 kg)。血清中峰浓度和谷浓度的中位数(范围)分别为20.16(4.40 - 69.00)mg/L和2.54(0.00 - 31.40)mg/L。CSF中相应的峰浓度和谷浓度分别为1.20(0.00 - 6.20)mg/L和1.28(0.00 - 4.10)mg/L,CSF/血清比值中位数(范围)为0.09(0.03 - 0.16)。肌酐清除率中位数为60.7至217.6 ml/分钟(中位数122.5 ml/分钟)。三室线性群体药代动力学模型最为合适。对于任何模型参数,均无法支持协变量关系。美罗培南在CSF中的穿透性较差,CSF/血清比值中位数为9%,个体间药代动力学变异性较高。
对于患有脑室炎的神经重症监护患者,应考虑给予高于标准剂量的美罗培南,并进行血清和CSF的治疗药物监测,以实现美罗培南给药的个体化。