Institute of Primary Care, University of Zurich, University Hospital Zurich, Pestalozzistrasse 24, 8091, Zurich, Switzerland.
Institute of Primary and Community Care, Lucerne, Switzerland.
BMC Geriatr. 2020 Nov 16;20(1):471. doi: 10.1186/s12877-020-01870-8.
Management of patients with polypharmacy is challenging, and evidence for beneficial effects of deprescribing interventions is mixed. This study aimed to investigate whether a patient-centred deprescribing intervention of PCPs results in a reduction of polypharmacy, without increasing the number of adverse disease events and reducing the quality of life, among their older multimorbid patients.
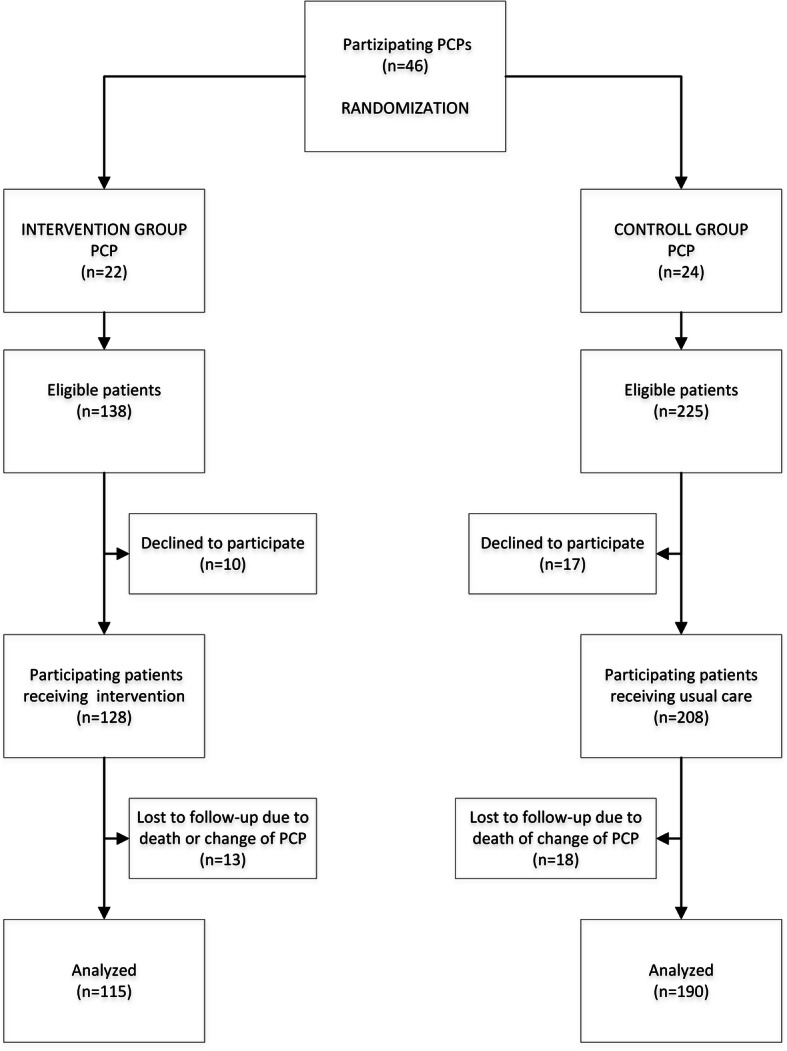
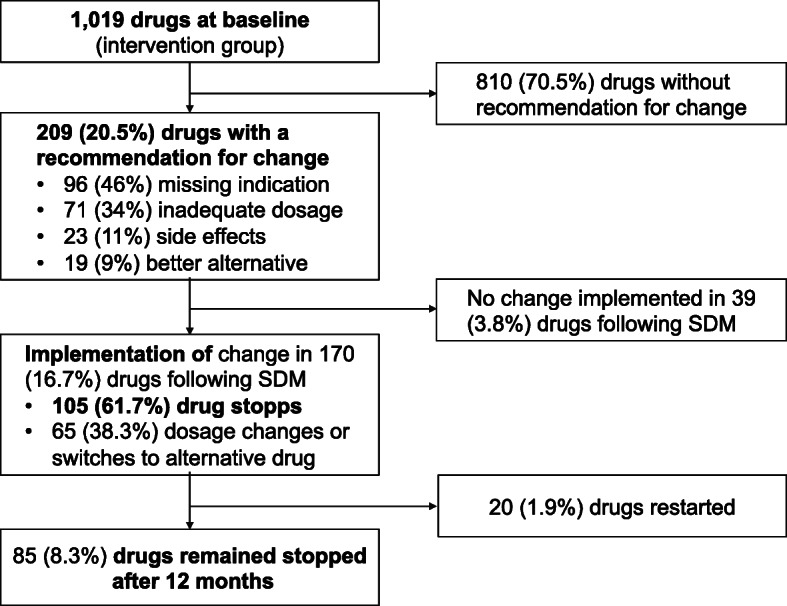
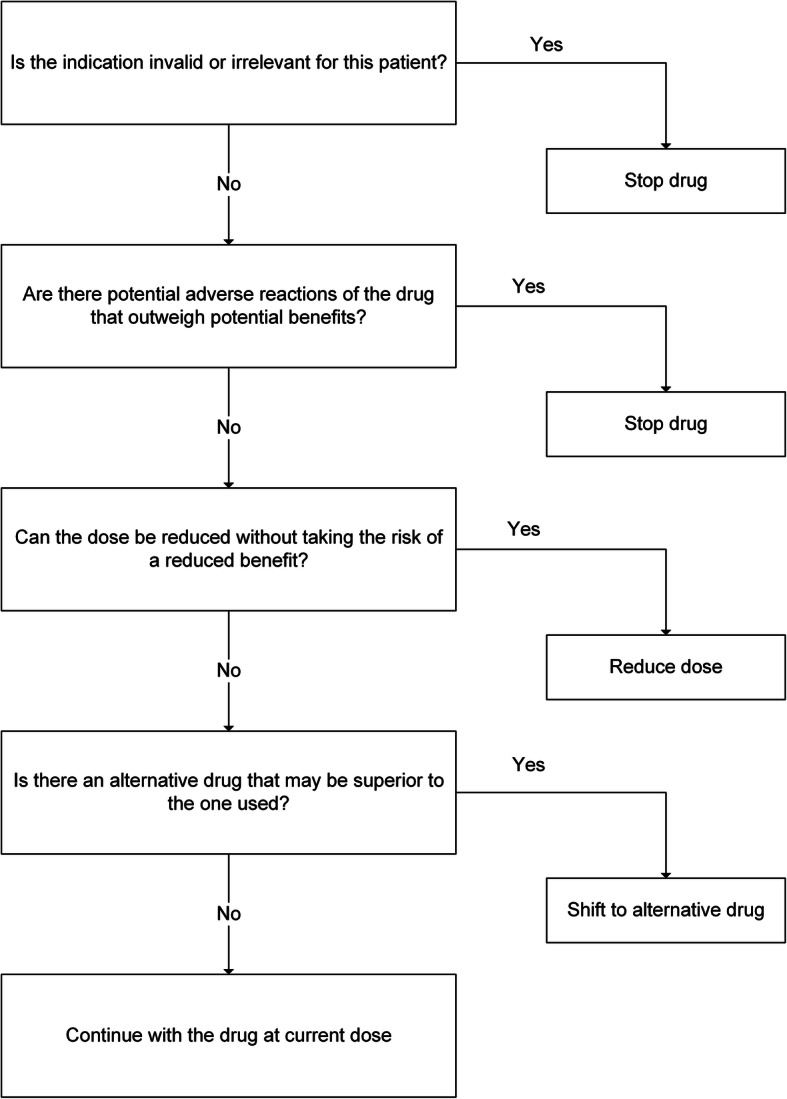
This is a cluster-randomised clinical study among 46 primary care physicians (PCPs) with a 12 months follow-up. We randomised PCPs into an intervention and a control group. They recruited 128 and 206 patients if ≥60 years and taking ≥five drugs for ≥6 months. The intervention consisted of a 2-h training of PCPs, encouraging the use of a validated deprescribing-algorithm including shared-decision-making, in comparison to usual care. The primary outcome was the mean difference in the number of drugs per patient (dpp) between baseline and after 12 months. Additional outcomes focused on patient safety and quality of life (QoL) measures.
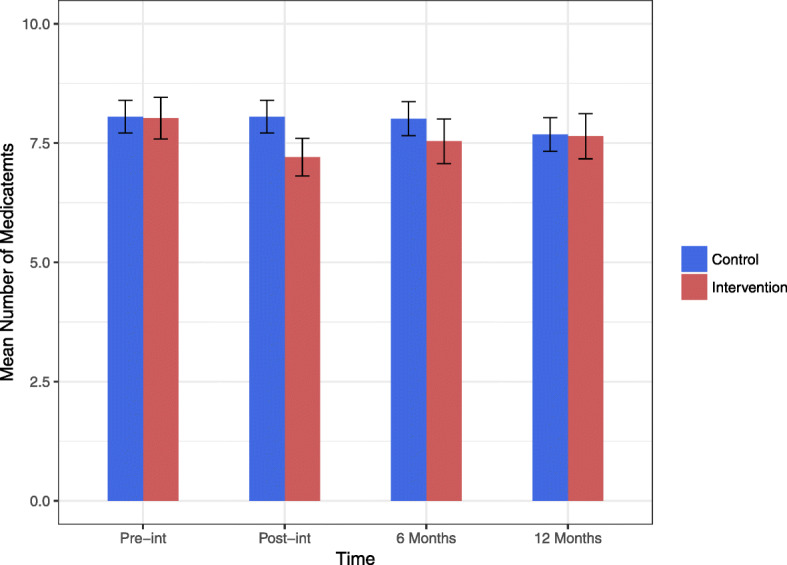
Three hundred thirty-four patients, mean [SD] age of 76.2 [8.5] years participated. The mean difference in the number of dpp between baseline and after 12 months was 0.379 in the intervention group (8.02 and 7.64; p = 0.059) and 0.374 in the control group (8.05 and 7.68; p = 0.065). The between-group comparison showed no significant difference at all time points, except for immediately after the intervention (p = 0.002). There were no significant differences concerning patient safety nor QoL measures.
Our straight-forward and patient-centred deprescribing procedure is effective immediately after the intervention, but not after 6 and 12 months. Further research needs to determine the optimal interval of repeated deprescribing interventions for a sustainable effect on polypharmacy at mid- and long-term. Integrating SDM in the deprescribing process is a key factor for success.
Current Controlled Trials, prospectively registered ISRCTN16560559 Date assigned 31/10/2014. The Prevention of Polypharmacy in Primary Care Patients Trial (4P-RCT).
管理同时服用多种药物的患者具有挑战性,且有关减少药物治疗的干预措施有益效果的证据不一。本研究旨在调查初级保健医生(PCP)实施以患者为中心的减少药物治疗方案是否会减少多药治疗,同时不增加不良疾病事件的数量和降低生活质量,对象为年龄较大且患有多种疾病的患者。
这是一项针对 46 名初级保健医生(PCP)的聚类随机临床试验,随访时间为 12 个月。我们将 PCP 随机分为干预组和对照组。如果患者年龄≥60 岁且服用≥5 种药物≥6 个月,则他们分别招募 128 名和 206 名患者。干预措施包括对 PCP 进行 2 小时的培训,鼓励使用经过验证的减少药物治疗算法,包括共享决策,与常规护理进行比较。主要结局是患者在基线和 12 个月后的药物数量的平均值差异(dpp)。其他结局主要关注患者安全性和生活质量(QoL)测量。
共有 334 名患者参与,平均年龄为 76.2 [8.5] 岁。干预组在基线和 12 个月后 dpp 的平均差异为 0.379(8.02 和 7.64;p=0.059),对照组为 0.374(8.05 和 7.68;p=0.065)。除了干预后立即(p=0.002)外,两组在所有时间点均无显著差异。患者安全性和 QoL 测量也没有显著差异。
我们简单直接且以患者为中心的减少药物治疗程序在干预后立即有效,但在 6 个月和 12 个月后无效。需要进一步研究确定重复减少药物治疗干预的最佳间隔时间,以实现多药治疗的中短期可持续效果。在减少药物治疗过程中整合共享决策是成功的关键因素。
当前对照试验,前瞻性注册 ISRCTN62313447 日期分配 2014 年 10 月 31 日。初级保健患者多药治疗预防试验(4P-RCT)。