Department of Surgery, Sol Goldman Pancreatic Cancer Research Center, Johns Hopkins University School of Medicine, Baltimore, MD.
Department of Pathology, Washington University, Saint Louis, MO.
Ann Surg. 2022 Aug 1;276(2):370-377. doi: 10.1097/SLA.0000000000004488. Epub 2020 Nov 17.
To define frequencies, pattern of progression (invasive vs noninvasive), and risk factors of progression of resected noninvasive intraductal papillary mucinous neoplasms (IPMNs).
There is a risk of progression in the remnant pancreas after resection of IPMNs.
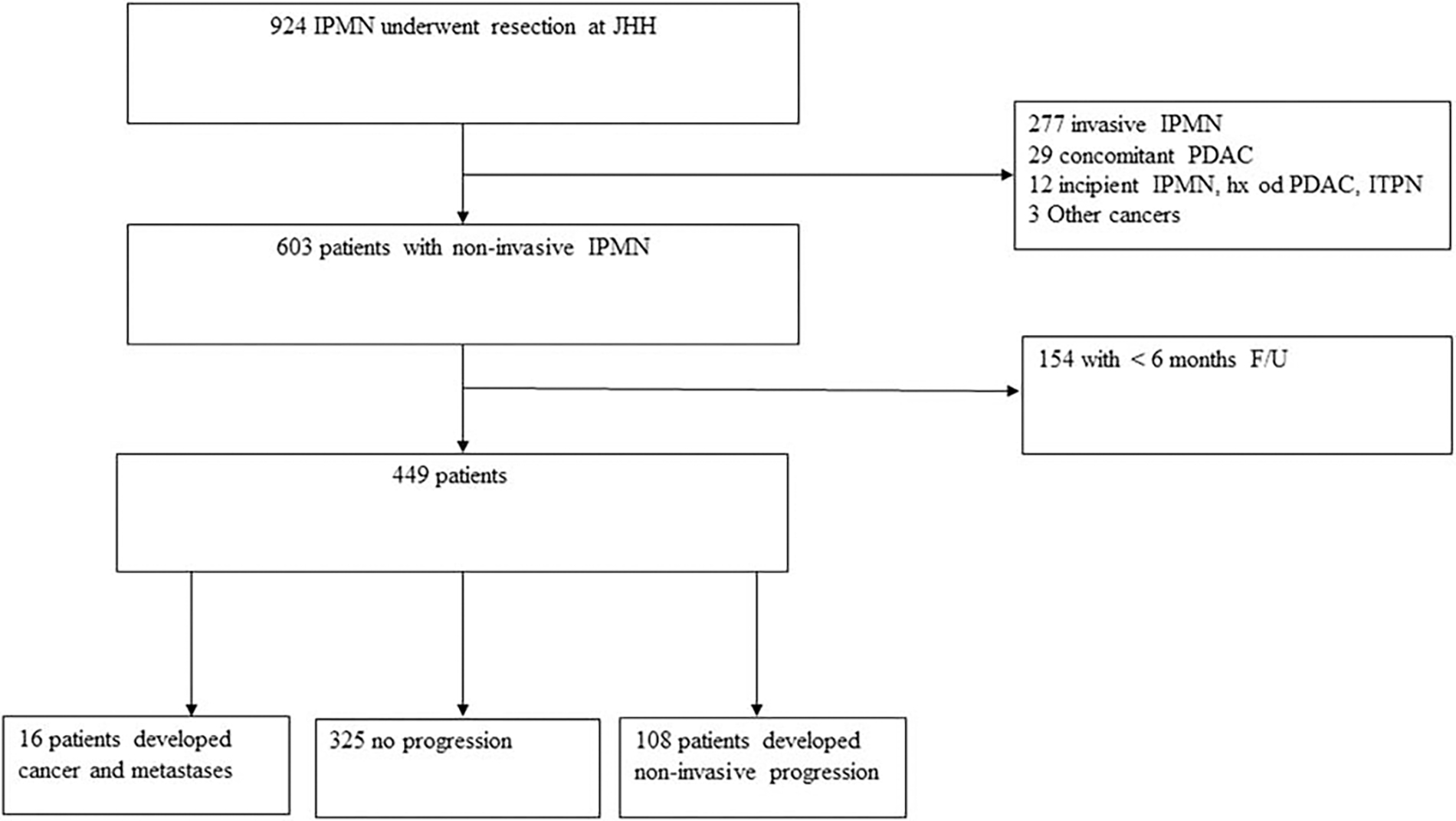
Four hundred forty-nine consecutive patients with resected IPMNs from 1995 to 2018 were included to the study. Patients with invasive carcinoma or with follow-up <6 months were excluded. Noninvasive progression was defined as a new IPMN, increased main pancreatic duct size, and increased size of an existing lesion (5 mm compared with preoperative imaging). Invasive progression was defined as development of invasive cancer in the remnant pancreas or metastatic disease.
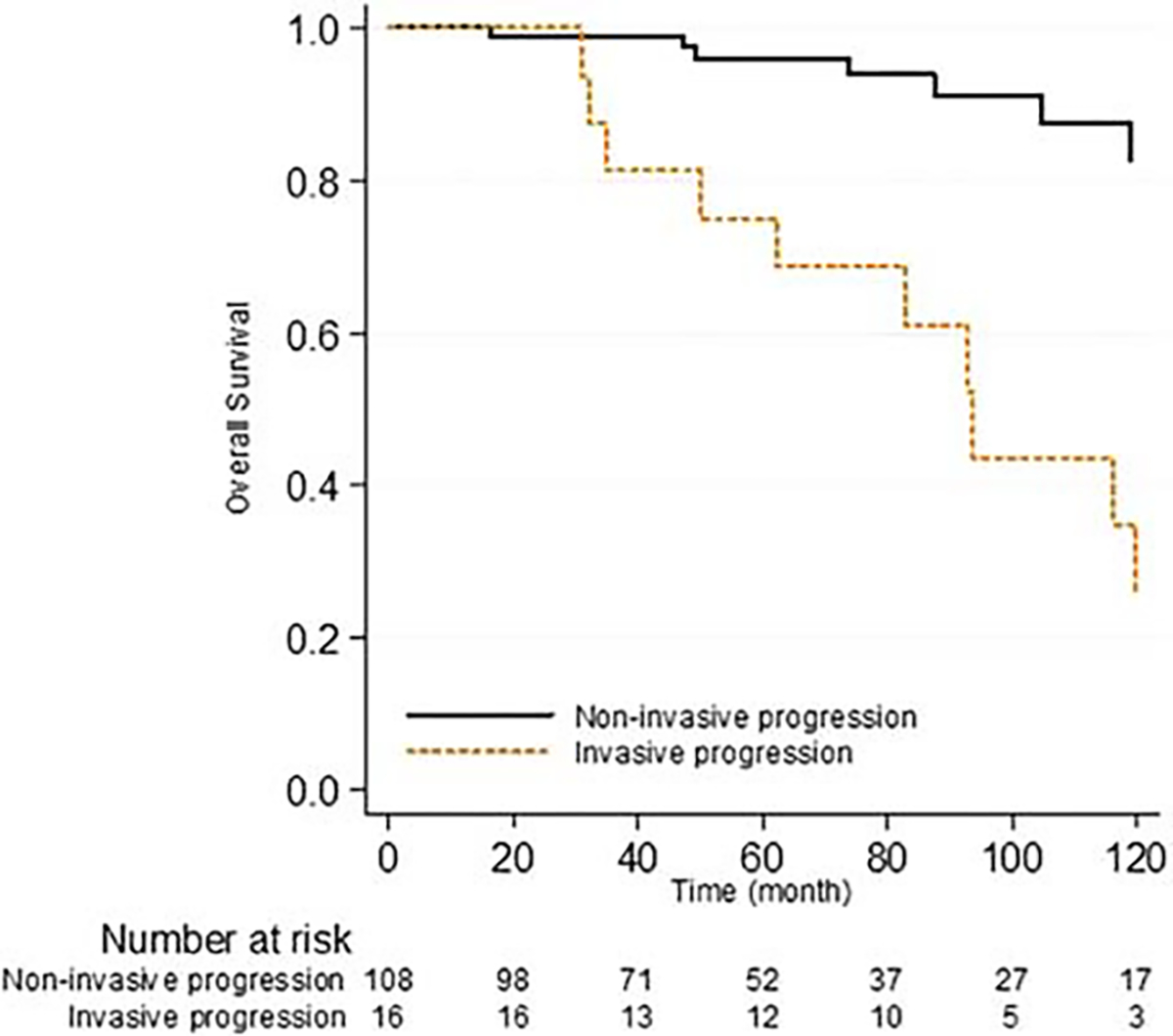
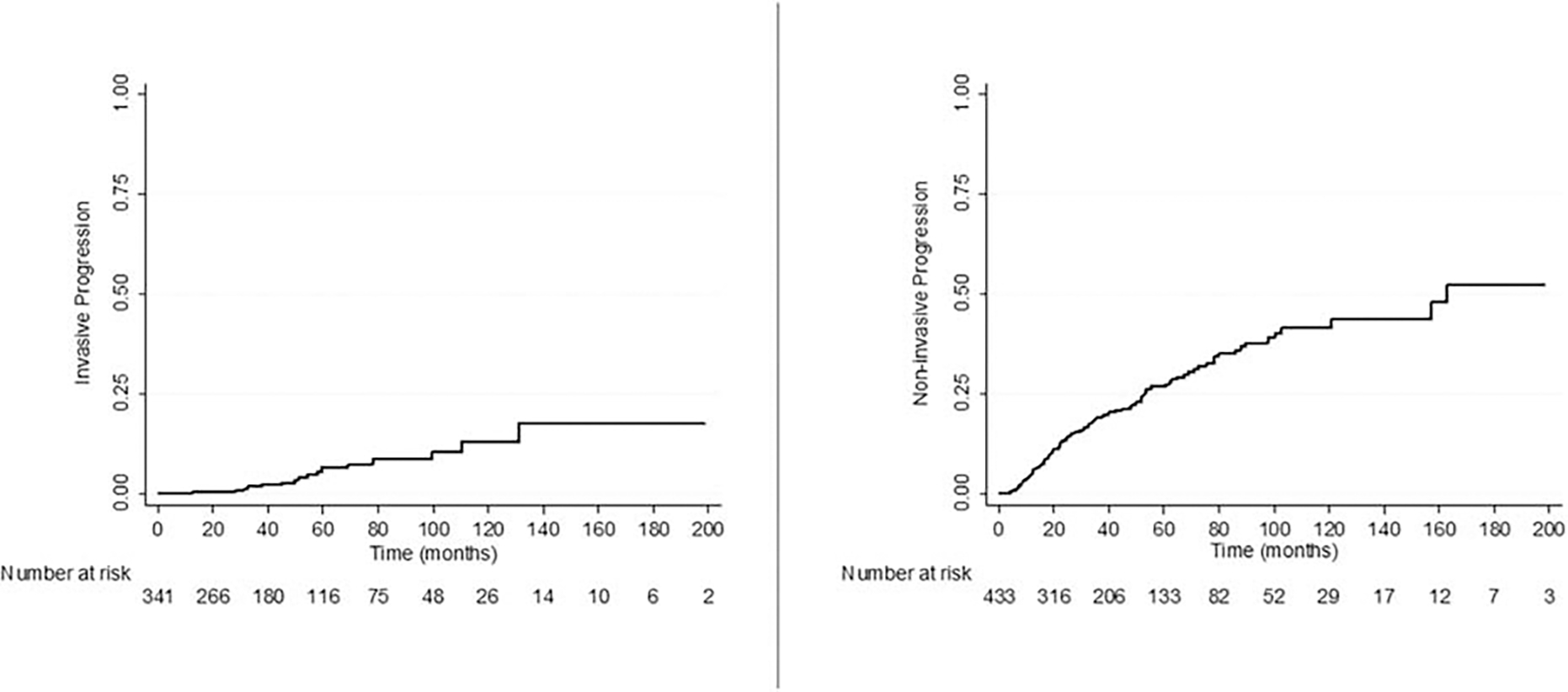
With a median follow-up of 48.9 months, progression was identified in 124 patients (27.6%); 108(24.1%) with noninvasive and 16(3.6%) with invasive progression. Median progression follow-up was longer for invasive progression (85.4 vs 55.9 months; P = 0.001). Five-and 10-year estimates for a cumulative incidence of invasive progression were 6.4% and 12.9% versus 26.9% and 41.5% for noninvasive progression. After risk adjustment, multifocality (HR 4.53, 95% CI 1.34-15.26; P = 0.02) and high-grade dysplasia (HGD) in the original resection (HR 3.60, 95% CI 1.13-11.48; P = 0.03) were associated with invasive progression.
Progression to invasive carcinoma can occur years after the surgical resection of a noninvasive IPMN. HGD in the original resection is a risk factor for invasive progression but some cases of low-grade dysplasia also progressed to cancer. Patients with high-risk features such as HGD and multifocal cysts should be considered for more intensive surveillance and represent an important cohort for future trials such as anti-inflammatory or prophylactic immunotherapy.
定义切除非浸润性导管内乳头状黏液性肿瘤(IPMN)后肿瘤进展的频率、模式(侵袭性与非侵袭性)和危险因素。
在切除 IPMN 后,胰腺残端有进展的风险。
本研究纳入了 1995 年至 2018 年间连续 449 例接受 IPMN 切除术的患者。排除了侵袭性癌患者或随访时间<6 个月的患者。非侵袭性进展定义为新发 IPMN、主胰管直径增大以及现有病变大小增加(与术前影像学相比增加 5mm)。侵袭性进展定义为胰腺残端发生浸润性癌或转移疾病。
中位随访 48.9 个月时,124 例患者(27.6%)出现进展,其中 108 例(24.1%)为非侵袭性进展,16 例(3.6%)为侵袭性进展。侵袭性进展的中位随访时间较长(85.4 个月 vs. 55.9 个月;P = 0.001)。侵袭性进展的 5 年和 10 年累积发生率分别为 6.4%和 12.9%,而非侵袭性进展分别为 26.9%和 41.5%。经风险调整后,多灶性(HR 4.53,95%CI 1.34-15.26;P = 0.02)和原发切除组织中高级别异型增生(HGD)(HR 3.60,95%CI 1.13-11.48;P = 0.03)与侵袭性进展相关。
在切除非浸润性 IPMN 多年后,可能会发生浸润性癌。原发切除组织中的 HGD 是侵袭性进展的危险因素,但有些低级别异型增生的病例也进展为癌症。具有 HGD 和多灶性囊肿等高危特征的患者应考虑进行更密集的监测,这些患者是未来抗炎或预防性免疫治疗等临床试验的重要队列。