School of Rehabilitation, Faculty of Medicine and Health Sciences, Pavillon Gérald-Lasalle, Université de Sherbrooke, Sherbrooke, QC J1H 5N4, Canada.
Research Centre on Aging, Estrie Integrated University Health and Social Services Centre-Sherbrooke Hospital University Centre, Sherbrooke, QC J1H 4C4, Canada.
Int J Environ Res Public Health. 2020 Nov 13;17(22):8399. doi: 10.3390/ijerph17228399.
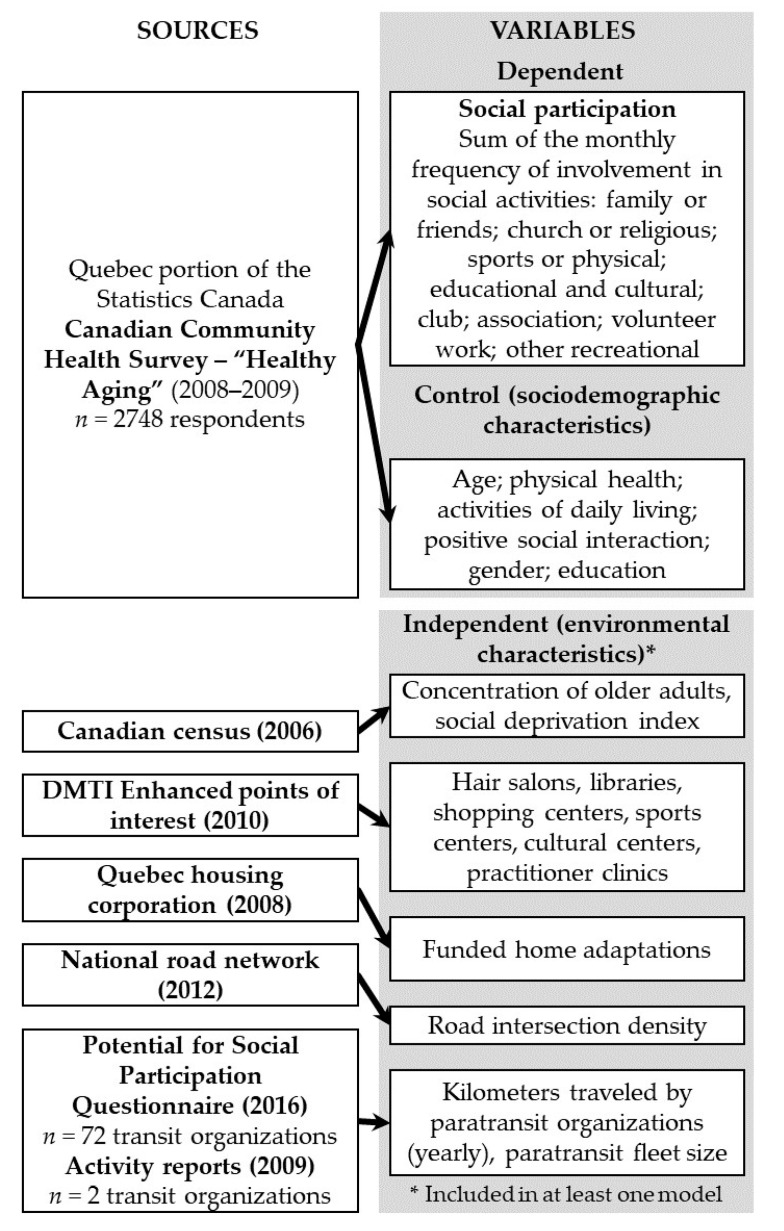
Although social participation fosters older adults' health, little is known about which environmental characteristics are related to greater participation in social activities. The Canadian Community Health Survey ( = 2737), a transportation survey, and multiple secondary data sources were used to identify the environmental characteristics associated with older Quebecers' social participation according to living area. Greater social participation was associated with: (1) a higher concentration of older adults (IRR = 2.172 (95% CI 1.600, 2.948); < 0.001), more kilometers traveled by paratransit (IRR = 1.714 (95% CI 1.286, 2.285); < 0.01), a lack of medical clinics (IRR = 0.730 (95% CI 0.574, 0.930); = 0.01), and more funded home adaptations (IRR = 1.170 (95% CI 1.036, 1.320); = 0.01) in large metropolitan areas; (2) larger paratransit fleets (IRR = 1.368 (95% CI 1.044, 1.791); = 0.02) and a lower density of road intersections (IRR = 0.862 (95% CI 0.756, 0.982); = 0.03) in regular metropolitan areas; (3) less social deprivation (IRR = 1.162 (95% CI 1.025, 1.318); = 0.02) in urban areas; and (4) a higher concentration of older populations (IRR = 2.386 (95% CI 1.817, 3.133); < 0.001) in rural areas. According to these findings, social participation interventions should target the local environment-for example, by providing more social interaction opportunities for older adults living in younger neighborhoods and by improving access to public transportation, especially paratransit.
尽管社会参与促进了老年人的健康,但人们对哪些环境特征与更多的社会活动参与有关知之甚少。利用加拿大社区健康调查(=2737)、交通调查和多个二级数据源,根据居住区域确定了与魁北克省老年人社会参与相关的环境特征。更高的社会参与与以下因素相关:(1)老年人的高度集中(IRR=2.172(95%CI 1.600, 2.948);<0.001)、更多的辅助交通出行里程(IRR=1.714(95%CI 1.286, 2.285);<0.01)、缺乏医疗诊所(IRR=0.730(95%CI 0.574, 0.930);=0.01)和更多的资助家庭适应(IRR=1.170(95%CI 1.036, 1.320);=0.01)在大都市区;(2)更大的辅助交通车队(IRR=1.368(95%CI 1.044, 1.791);=0.02)和更低的道路交叉口密度(IRR=0.862(95%CI 0.756, 0.982);=0.03)在常规大都市区;(3)在城市地区社会贫困程度较低(IRR=1.162(95%CI 1.025, 1.318);=0.02);(4)农村地区老年人口高度集中(IRR=2.386(95%CI 1.817, 3.133);<0.001)。根据这些发现,社会参与干预措施应该针对当地环境,例如,为居住在较年轻社区的老年人提供更多的社会互动机会,并改善公共交通,特别是辅助交通的可达性。