London Centre for Neglected Tropical Disease Research, London, UK.
Department of Infectious Disease Epidemiology, School of Public Health, Faculty of Medicine, St Mary's Campus, Imperial College London, London, UK.
Parasit Vectors. 2020 Nov 18;13(1):554. doi: 10.1186/s13071-020-04409-3.
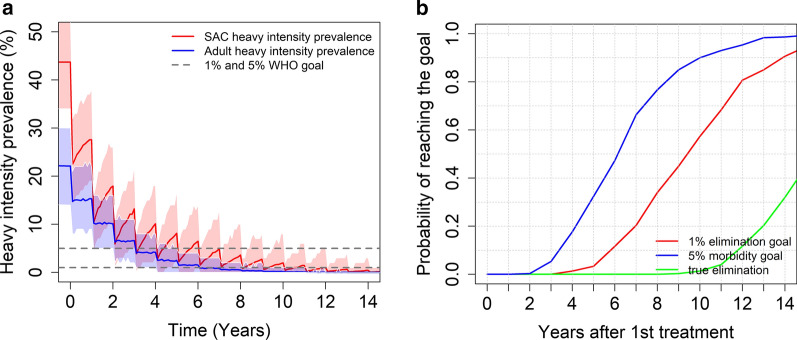
Schistosomiasis remains an endemic parasitic disease causing much morbidity and, in some cases, mortality. The World Health Organization (WHO) has outlined strategies and goals to combat the burden of disease caused by schistosomiasis. The first goal is morbidity control, which is defined by achieving less than 5% prevalence of heavy intensity infection in school-aged children (SAC). The second goal is elimination as a public health problem (EPHP), achieved when the prevalence of heavy intensity infection in SAC is reduced to less than 1%. Mass drug administration (MDA) of praziquantel is the main strategy for control. However, there is limited availability of praziquantel, particularly in Africa where there is high prevalence of infection. It is therefore important to explore whether the WHO goals can be achieved using the current guidelines for treatment based on targeting SAC and, in some cases, adults. Previous modelling work has largely focused on Schistosoma mansoni, which in advance cases can cause liver and spleen enlargement. There has been much less modelling of the transmission of Schistosoma haematobium, which in severe cases can cause kidney damage and bladder cancer. This lack of modelling has largely been driven by limited data availability and challenges in interpreting these data.
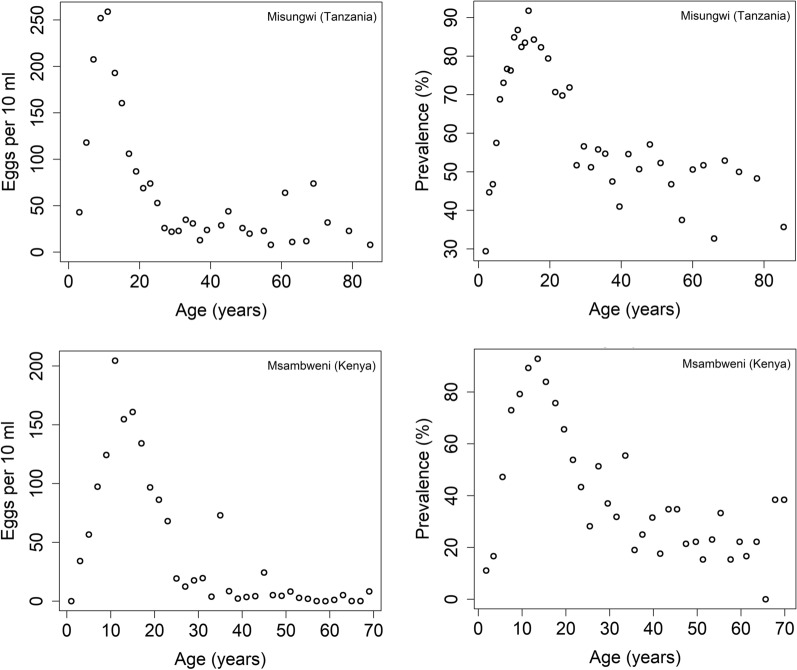
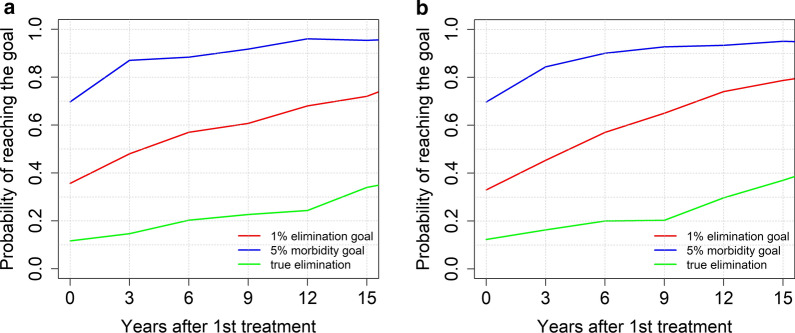
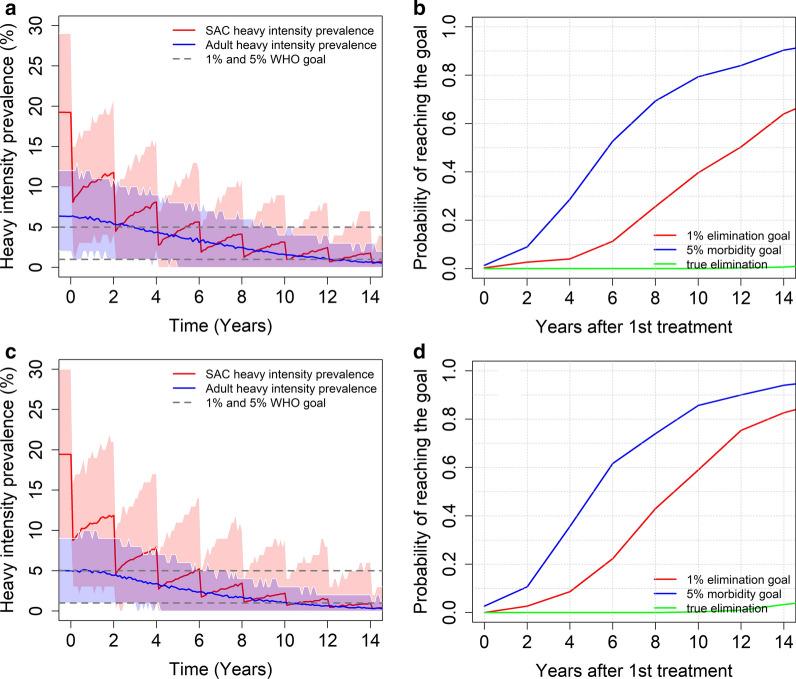
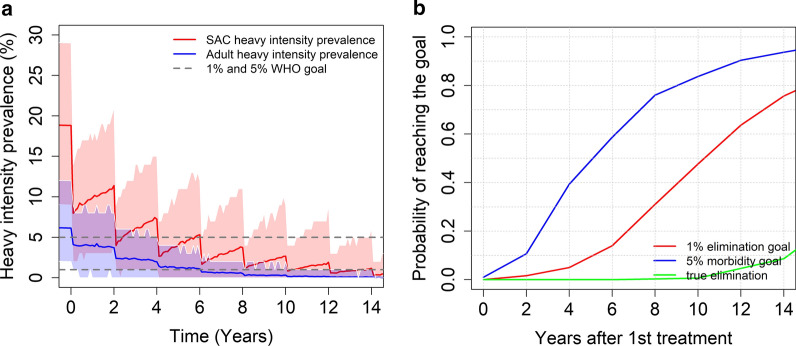
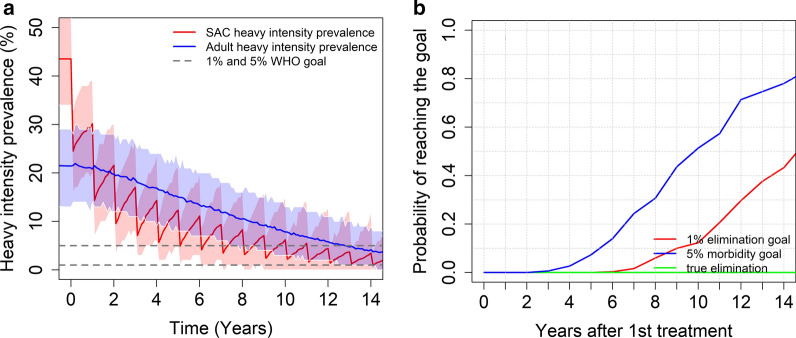
In this paper, using an individual-based stochastic model and age-intensity profiles of S. haematobium from two different communities, we calculate the probability of achieving the morbidity and EPHP goals within 15 years of treatment under the current WHO treatment guidelines. We find that targeting SAC only can achieve the morbidity goal for all transmission settings, regardless of the burden of infection in adults. The EPHP goal can be achieved in low transmission settings, but in some moderate to high settings community-wide treatment is needed.
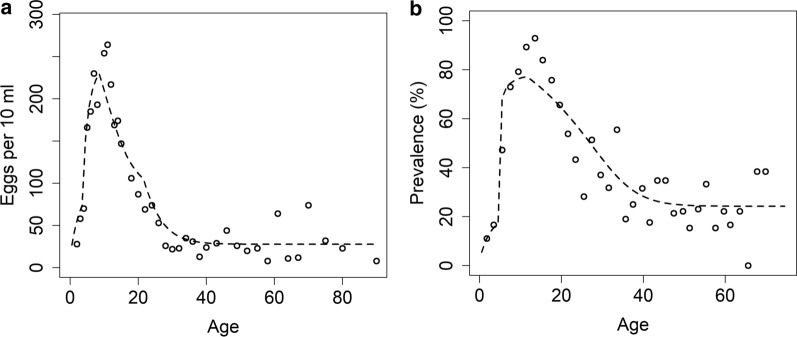
We show that the key determinants of achieving the WHO goals are the precise form of the age-intensity of infection profile and the baseline SAC prevalence. Additionally, we find that the higher the burden of infection in adults, the higher the chances that adults need to be included in the treatment programme to achieve EPHP.
血吸虫病仍然是一种地方性寄生虫病,导致大量发病,在某些情况下还会导致死亡。世界卫生组织(WHO)已经概述了抗击血吸虫病负担的战略和目标。第一个目标是控制发病率,其定义为在校儿童(SAC)中重度感染的流行率低于 5%。第二个目标是消除作为公共卫生问题(EPHP),当 SAC 中的重度感染流行率降低到低于 1%时即可实现。吡喹酮大规模药物治疗(MDA)是控制的主要策略。然而,吡喹酮的供应有限,特别是在感染率高的非洲地区。因此,重要的是要探索是否可以使用针对 SAC 并在某些情况下针对成年人的现行治疗指南来实现世卫组织的目标。以前的建模工作主要集中在曼氏血吸虫上,在晚期病例中,曼氏血吸虫会导致肝脾肿大。对埃及血吸虫的传播的建模要少得多,在严重情况下,埃及血吸虫会导致肾脏损伤和膀胱癌。这种建模的缺乏主要是由于数据可用性有限以及解释这些数据的挑战所致。
在本文中,我们使用基于个体的随机模型和来自两个不同社区的埃及血吸虫年龄-强度曲线,根据现行的世卫组织治疗指南,计算了在治疗后 15 年内达到发病率和 EPHP 目标的概率。我们发现,仅针对 SAC 可以实现所有传播环境下的发病率目标,而与成年人的感染负担无关。在低传播环境下可以实现 EPHP 目标,但在一些中等到高传播环境下需要进行全社区治疗。
我们表明,实现世卫组织目标的关键决定因素是感染的精确年龄-强度曲线形式和 SAC 的基线流行率。此外,我们发现,成年人的感染负担越高,成年人需要纳入治疗计划以实现 EPHP 的可能性就越高。