Dasic Davor, Rath Narendra K, Ganau Mario, Sarsam Zaid
Department of Neurosurgery, The Walton Centre NHS Foundation Trust, Liverpool, UK.
Department of Neurosurgery, Oxford University Hospitals NHS Foundation Trust, Oxford, UK.
Case Rep Surg. 2020 Nov 1;2020:8891021. doi: 10.1155/2020/8891021. eCollection 2020.
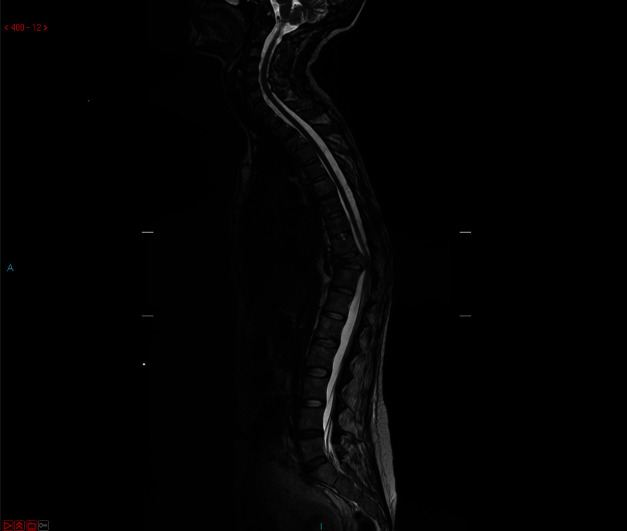
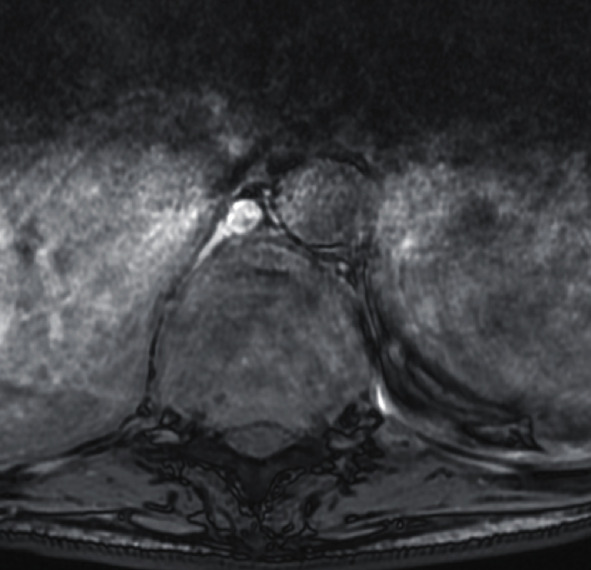
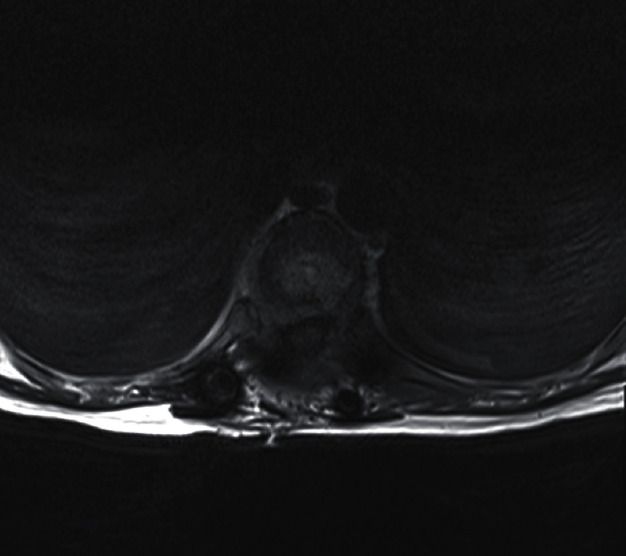
Primary and secondary spinal tumours with cord compression often represent a challenging condition for the patient and clinicians alike, even more so during pregnancy. The balance between safe delivery of a healthy baby and management of the mother's disease bears many clinical, psychological, and ethical dilemmas. Pregnancy sets a conflict between the optimal surgical and oncological managements of the mother's tumour and the well-being of her foetus. We followed the CARE guidelines from the EQUATOR Network to report an exemplificative case of a 39-year-old woman with a 10-year history of breast cancer, presenting in the second trimester of her first pregnancy with acute onset severe thoracic spinal instability, causing mechanical pain and weakness in lower limbs. Neuroradiological investigations revealed multilevel spinal deposits with a pathological T10 fracture responsible for spinal cord compression. The patient was adamant that she wanted a continuation of the pregnancy and her baby delivered. After discussion with her oncologist and obstetrician, we agreed to perform emergency spinal surgery-decompression and instrumented fixation. The literature search did not reveal a similar case of spinal metastatic breast cancer undergoing spinal instrumentation and delivery of a healthy baby a few months later. Following the delivery, the patient had further oncological treatment, including chemotherapy and radiotherapy. The paucity of such reports prompted us to present this case and highlight the relevance of a multidisciplinary approach involving obstetrician, oncologist, spinal surgeon, and radiologist to guide the optimal decision-making process.
伴有脊髓压迫的原发性和继发性脊柱肿瘤,对患者和临床医生来说往往都是具有挑战性的情况,在孕期更是如此。在安全分娩健康婴儿与治疗母亲疾病之间寻求平衡,存在诸多临床、心理和伦理困境。怀孕使得母亲肿瘤的最佳手术和肿瘤治疗管理与胎儿的健康之间产生了冲突。我们遵循赤道网络的CARE指南,报告一例典型病例:一名39岁女性,有10年乳腺癌病史,在其首次怀孕的中期出现急性严重胸段脊柱不稳,导致机械性疼痛和下肢无力。神经放射学检查发现多处脊柱转移灶,伴有病理性T10骨折,导致脊髓受压。患者坚决要求继续妊娠并分娩婴儿。在与她的肿瘤学家和产科医生讨论后,我们同意进行急诊脊柱手术——减压和器械固定。文献检索未发现类似的脊柱转移性乳腺癌病例,该病例接受了脊柱内固定术,并在几个月后分娩出健康婴儿。分娩后,患者接受了进一步的肿瘤治疗,包括化疗和放疗。此类报告的匮乏促使我们呈现该病例,并强调多学科方法(包括产科医生、肿瘤学家、脊柱外科医生和放射科医生)对于指导最佳决策过程的相关性。