Khalil Melissa, Karimzad Kaveh, Durand Jean-Bernard, Malek Alexandre E, Raad Issam I, Viola George M
Department of Infectious Diseases, The University of Texas MD Anderson Cancer Center, Houston, Texas, USA.
Department of Cardiology, The University of Texas MD Anderson Cancer Center, Houston, Texas, USA.
Open Forum Infect Dis. 2020 Sep 13;7(11):ofaa433. doi: 10.1093/ofid/ofaa433. eCollection 2020 Nov.
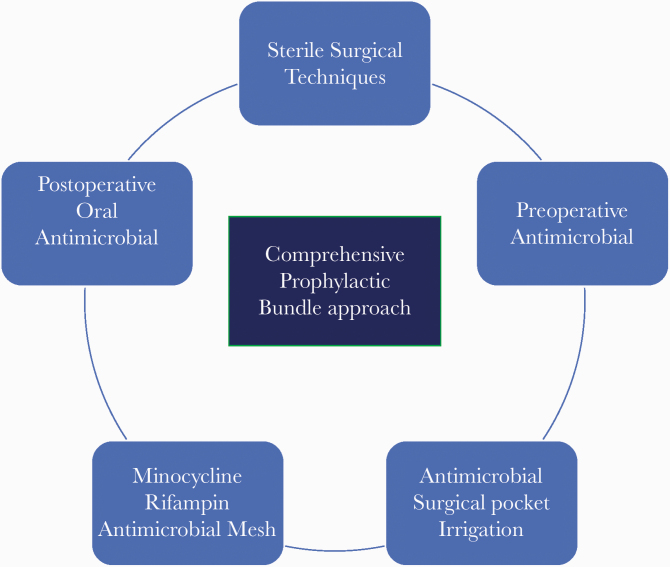
Oncological patients have several additional risk factors for developing a cardiac implantable electronic device (CIED)-related infection. Therefore, we evaluated the clinical impact of our comprehensive bundle approach that includes the novel minocycline and rifampin antimicrobial mesh (TYRX) for the prevention of CIED infections in patients living with cancer.
We retrospectively reviewed all consecutive patients who had a CIED placement at our institution during 2012-2017 who received preoperative vancomycin, intraoperative pocket irrigation with bacitracin and polymyxin B, plus TYRX antimicrobial mesh, followed by postoperative oral minocycline.
A total of 154 patients had a CIED, with 97 permanent pacemakers (PPMs), 23 implantable cardioverter defibrillators (ICDs), and 34 cardiac resynchronization therapy (CRT) devices. An underlying solid cancer was present in 62% of patients, while 38% had a hematologic malignancy. Apart from a higher proportion of surgical interventions in the PPM group than in the ICD and CRT groups ( = .007), no other oncologic variables were statistically significantly different between groups. Despite an extensive median follow-up period (interquartile range) of 21.9 (6.7-33.8) months, 16 patients (10%) had a mechanical complication, while only 2 patients (1.3%) developed a CIED infection, requiring the device to be explanted.
Our comprehensive prophylactic bundle approach using TYRX antimicrobial mesh in an oncologic population at high risk for infections was revealed upon extensive follow-up to be both safe and effective in maintaining the rate of CIED infection at 1.3%, well within published averages in the broader population of CIED recipients.
肿瘤患者发生心脏植入式电子设备(CIED)相关感染的风险因素更多。因此,我们评估了我们的综合方案的临床效果,该方案包括新型米诺环素和利福平抗菌网(TYRX),用于预防癌症患者的CIED感染。
我们回顾性分析了2012年至2017年期间在我们机构接受CIED植入的所有连续患者,这些患者术前接受万古霉素治疗,术中用杆菌肽和多粘菌素B进行囊袋冲洗,并使用TYRX抗菌网,术后口服米诺环素。
共有154例患者植入了CIED,其中97例为永久性起搏器(PPM),23例为植入式心脏复律除颤器(ICD),34例为心脏再同步治疗(CRT)设备。62%的患者患有实体癌,38%的患者患有血液系统恶性肿瘤。除PPM组的手术干预比例高于ICD组和CRT组外(P = 0.007),各组间其他肿瘤学变量无统计学显著差异。尽管中位随访期较长(四分位间距),为21.9(6.7 - 33.8)个月,但16例患者(10%)出现机械并发症,只有2例患者(1.3%)发生CIED感染,需要取出设备。
我们在高感染风险的肿瘤患者中使用TYRX抗菌网的综合预防方案,经过广泛随访发现,在将CIED感染率维持在1.3%方面既安全又有效,该感染率远低于CIED接受者更广泛人群中公布的平均水平。