DuBrock Hilary M, Runo James R, Sadd Corey J, Burger Charles D, Cartin-Ceba Rodrigo, Rosen Charles B, Taner Timucin, Nyberg Scott L, Heimbach Julie K, Findlay James Y, Krowka Michael J
Division of Pulmonary and Critical Care, Mayo Clinic, Rochester, MN.
Division of Pulmonary and Critical Care, University of Wisconsin, Madison, WI.
Transplant Direct. 2020 Nov 10;6(12):e630. doi: 10.1097/TXD.0000000000001085. eCollection 2020 Dec.
Portopulmonary hypertension (POPH), pulmonary arterial hypertension (PAH) that develops in the setting of portal hypertension, affects 5%-6% of patients with liver disease and is associated with significant morbidity and mortality. A mean pulmonary arterial pressure (mPAP) threshold of 35 mm Hg is used to stratify perioperative risk and liver transplant eligibility in treated POPH patients but does not take into account the specific factors that contribute to the pressure elevation.
In this case series, we describe the characteristics and posttransplant outcomes of patients with treated POPH and an mPAP ≥35 mm Hg and pulmonary vascular resistance (PVR) <250 dynes-s-cm at or just before liver transplantation (LT). We also describe the effect of PAH therapy on pulmonary hemodynamics in patients with POPH.
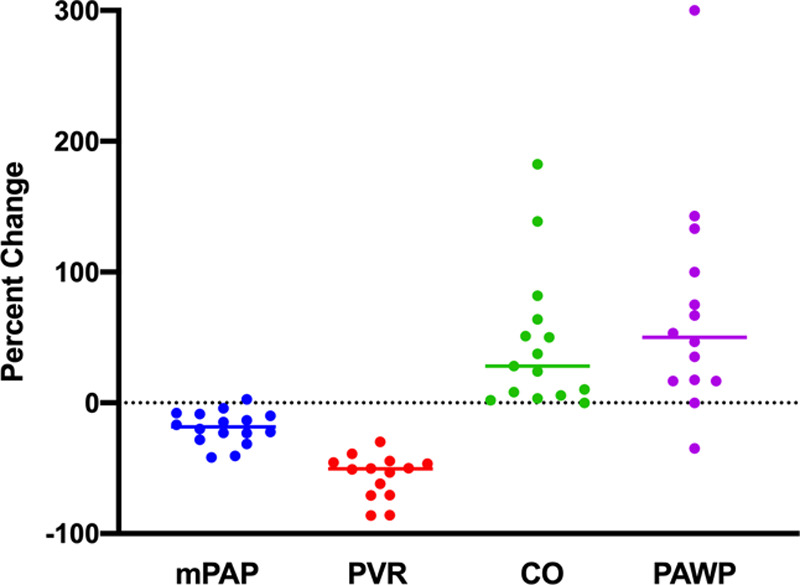
Sixteen patients were included. All patients were on PAH therapy at the time of LT. PAH therapy resulted in a decrease of mPAP (median 18.4%; interquartile range [IQR] 8.9%-27.0%) with a reduction in PVR (median 50.5%; IQR, 45.4%-70.7%), and an increase in both cardiac output (CO) (median 28.1%; IQR 5.7%-63.8%) and PAWP (median 50.0%; IQR 16.7%-108.3%) before LT. One year posttransplant survival was 69% (11/16); however, only 1 death was attributed to POPH. At 1-year posttransplant, 63.6% (7/11) of patients were weaned off all PAH therapy with clinical and echocardiographic resolution of POPH.
In treated POPH patients with an mPAP ≥35 mm Hg and PVR < 250 dynes-s-cm before LT, 1-year posttransplant survival was 69% and the majority of patients were able to discontinue PAH therapy.
门肺高压(POPH)是在门静脉高压背景下发生的肺动脉高压(PAH),影响5% - 6%的肝病患者,且与显著的发病率和死亡率相关。35 mmHg的平均肺动脉压(mPAP)阈值用于对接受治疗的POPH患者的围手术期风险和肝移植资格进行分层,但未考虑导致压力升高的具体因素。
在这个病例系列中,我们描述了接受治疗的POPH患者在肝移植(LT)时或即将进行肝移植时mPAP≥35 mmHg且肺血管阻力(PVR)<250 dynes·s/cm的患者的特征和移植后结局。我们还描述了PAH治疗对POPH患者肺血流动力学的影响。
纳入16例患者。所有患者在LT时均接受PAH治疗。PAH治疗导致LT前mPAP降低(中位数18.4%;四分位间距[IQR] 8.9% - 27.0%),PVR降低(中位数50.5%;IQR,45.4% - 70.7%),心输出量(CO)增加(中位数28.1%;IQR 5.7% - 63.8%)以及肺动脉楔压(PAWP)增加(中位数50.0%;IQR 16.7% - 108.3%)。移植后1年生存率为69%(11/16);然而,仅1例死亡归因于POPH。移植后1年时,63.6%(7/11)的患者停用了所有PAH治疗,POPH在临床和超声心动图检查方面得到缓解。
在LT前mPAP≥35 mmHg且PVR < 250 dynes·s/cm的接受治疗的POPH患者中,移植后1年生存率为69%,且大多数患者能够停用PAH治疗。