Sahay Sandeep, Al Abdi Sami, Melillo Celia, Newman Jennie, Dweik Raed A, Heresi Gustavo A, Tonelli Adriano R
Weill Cornell Medical College, Institute of Academic Medicine, Houston Methodist Lung Center, Houston Methodist Hospital, Houston, TX.
Inflammation and Immunity Department, Lerner Research Institute, Cleveland Clinic, Cleveland, OH.
Transplant Direct. 2021 Jun 8;7(7):e710. doi: 10.1097/TXD.0000000000001162. eCollection 2021 Jul.
The causes and circumstances surrounding death are poorly studied in patients with portopulmonary hypertension (PoPH). We sought to determine the specific reasons for dying and characteristics surrounding this process in patients with PoPH.
All deaths of patients with PoPH followed in the Cleveland Clinic Pulmonary Vascular Program were prospectively reviewed by the pulmonary hypertension team between 1996 and 2020.
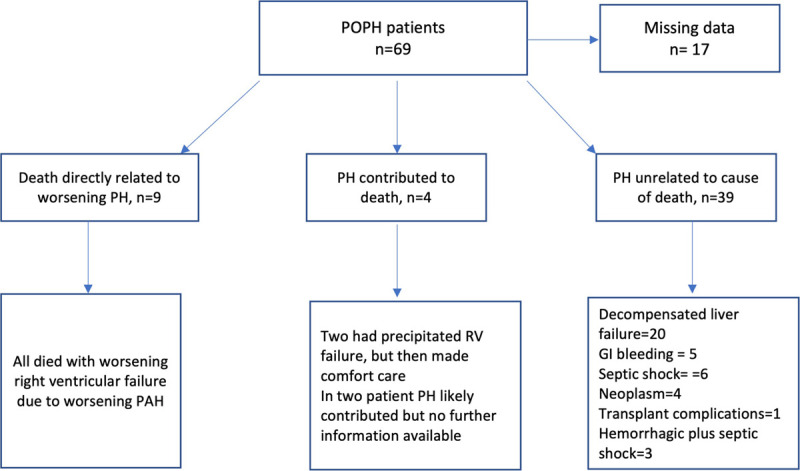
A total of 69 patients with PoPH (age 56.0 ± 8.9 y), with 49% females, were included. Causes of death were available in 52 (75%) patients, of these PoPH either directly or indirectly contributed to death in 13 of 52 (25%) of patients, meanwhile 39 of 52 (75%) of the patients died because of progressive liver disease and its related complications. Decompensated liver disease was the leading cause of death in this cohort 20 of 52 (38%), whereas 19 of 52 (37%) died because of conditions associated with liver disease. About half, 36 of 69 (52%) of patients died in a healthcare environment and 23 of 36 (64%) during a hospitalization at Cleveland Clinic. A total of 59 of 69 (74%) of patients received pulmonary arterial hypertension (PAH)-specific therapies. Six patients died after liver transplantation (in 3 death was related to PAH-related complications). Most of the patients in this cohort of PoPH patients were considered unsuitable for liver transplantation for a variety of reasons. Advanced healthcare directives were available in only 28% of patients.
Most patients with PoPH died because of complications of their liver disease. PAH directly or indirectly contributed to death in a third of them. A quarter of them did not receive PAH-specific therapy before their death.
关于门肺高压(PoPH)患者死亡的原因及相关情况研究较少。我们试图确定PoPH患者死亡的具体原因及这一过程的相关特征。
1996年至2020年期间,克利夫兰诊所肺动脉项目中所有PoPH患者的死亡情况均由肺动脉高压团队进行前瞻性回顾。
共纳入69例PoPH患者(年龄56.0±8.9岁),其中49%为女性。52例(75%)患者有死亡原因记录,其中52例中的13例(25%)患者,PoPH直接或间接导致死亡,同时52例中的39例(75%)患者死于进展性肝病及其相关并发症。失代偿性肝病是该队列中主要的死亡原因,52例中有20例(38%),而52例中有19例(37%)死于与肝病相关的情况。约一半,即69例中的36例(52%)患者在医疗环境中死亡,其中36例中的23例(64%)在克利夫兰诊所住院期间死亡。69例患者中有59例(74%)接受了肺动脉高压(PAH)特异性治疗。6例患者在肝移植后死亡(其中3例死亡与PAH相关并发症有关)。由于各种原因,该PoPH患者队列中的大多数患者被认为不适合肝移植。只有28%的患者有生前预嘱。
大多数PoPH患者死于肝病并发症。PAH直接或间接导致其中三分之一患者死亡。四分之一患者在死亡前未接受PAH特异性治疗。