Department of Neurosurgery, University Medical Center Hamburg-Eppendorf, Martinistraße 52, 20246, Hamburg, Germany.
Institute for Stem Cell Biology and Regenerative Medicine, Stanford University School of Medicine, 265 Campus Drive, Stanford, CA, 94305, USA.
Eur J Trauma Emerg Surg. 2022 Dec;48(6):4451-4459. doi: 10.1007/s00068-020-01544-5. Epub 2020 Nov 18.
Based on the hypothesis that systemic inflammation contributes to secondary injury after initial traumatic brain injury (TBI), this study aims to describe the effect of splenectomy on mortality in trauma patients with TBI and splenic injury.
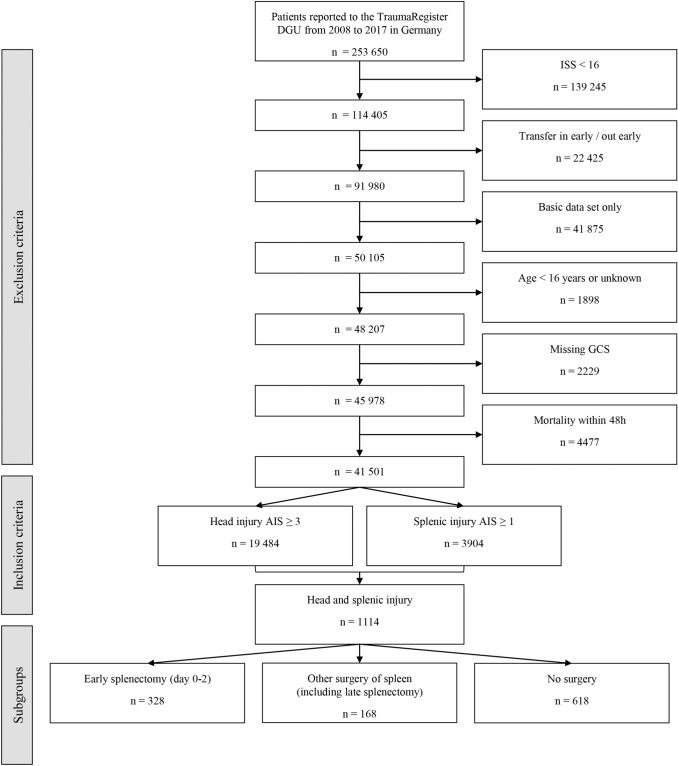
A retrospective cohort analysis of patients prospectively registered into the TraumaRegister DGU (TR-DGU) with TBI (AIS ≥ 3) combined with injury to the spleen (AIS ≥ 1) was conducted. Multivariable logistic regression modeling was performed to adjust for confounding factors and to assess the independent effect of splenectomy on in-hospital mortality.
The cohort consisted of 1114 patients out of which 328 (29.4%) had undergone early splenectomy. Patients with splenectomy demonstrated a higher Injury Severity Score (median: 34 vs. 44, p < 0.001) and lower Glasgow Coma Scale (median: 9 vs. 7, p = 0.014) upon admission. Splenectomized patients were more frequently hypotensive upon admission (19.8% vs. 38.0%, p < 0.001) and in need for blood transfusion (30.3% vs. 61.0%, p < 0.001). The mortality was 20.7% in the splenectomy group and 10.3% in the remaining cohort. After adjustment for confounding factors, early splenectomy was not found to exert a significant effect on in-hospital mortality (OR 1.29 (0.67-2.50), p = 0.45).
Trauma patients with TBI and spleen injury undergoing splenectomy demonstrate a more severe injury pattern, more compromised hemodynamic status and higher in-hospital mortality than patients without splenectomy. Adjustment for confounding factors reveals that the splenectomy procedure itself is not independently associated with survival.
基于全身炎症会导致原发性颅脑损伤(TBI)后继发性损伤的假设,本研究旨在描述脾切除术对合并 TBI 和脾损伤的创伤患者死亡率的影响。
对前瞻性登记于创伤登记处德国创伤协会(TR-DGU)的 TBI(AIS≥3)合并脾损伤(AIS≥1)的患者进行回顾性队列分析。采用多变量逻辑回归模型调整混杂因素,并评估脾切除术对住院死亡率的独立影响。
该队列包括 1114 例患者,其中 328 例(29.4%)接受了早期脾切除术。脾切除术患者的损伤严重程度评分(中位数:34 分比 44 分,p<0.001)和格拉斯哥昏迷评分(中位数:9 分比 7 分,p=0.014)入院时更高。脾切除患者入院时更常出现低血压(19.8%比 38.0%,p<0.001)和需要输血(30.3%比 61.0%,p<0.001)。脾切除术组死亡率为 20.7%,其余组为 10.3%。调整混杂因素后,早期脾切除术对住院死亡率无显著影响(OR 1.29(0.67-2.50),p=0.45)。
合并 TBI 和脾损伤的创伤患者行脾切除术的患者其损伤模式更严重,血流动力学状态更差,住院死亡率高于未行脾切除术的患者。调整混杂因素后发现,脾切除术本身与生存率无关。