Rosignoli Chiara, Petruzzellis Giuseppe, Radici Vera, Facchin Gabriele, Girgenti Marco, Stella Rossella, Isola Miriam, Battista Martalisa, Sperotto Alessandra, Geromin Antonella, Cerno Michela, Arzese Alessandra, Deias Paola, Tascini Carlo, Fanin Renato, Patriarca Francesca
Clinica Ematologica ed Unità di Terapie Cellulari, Azienda Sanitaria Universitaria Friuli Centrale, Piazzale S. Maria della Misericordia 10, 33100 Udine, Italy.
Istituto di Statistica, Dipartimento di Area Medica, Università di Udine, 33100 Udine, Italy.
J Clin Med. 2020 Nov 16;9(11):3673. doi: 10.3390/jcm9113673.
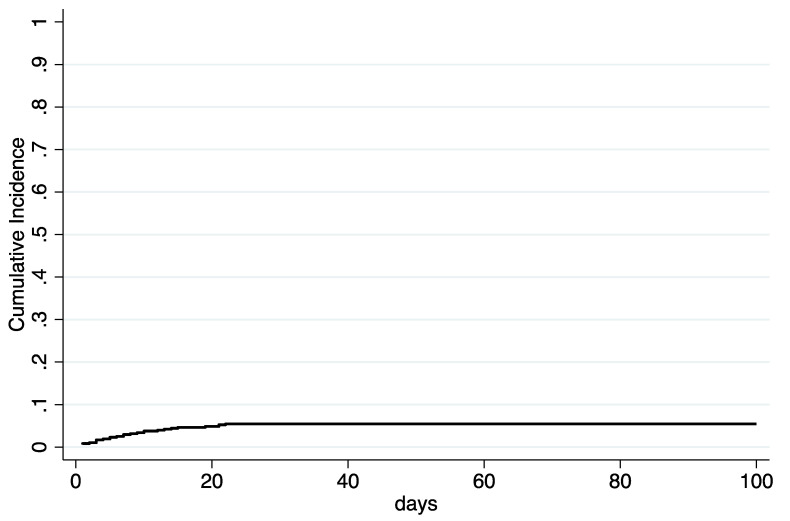
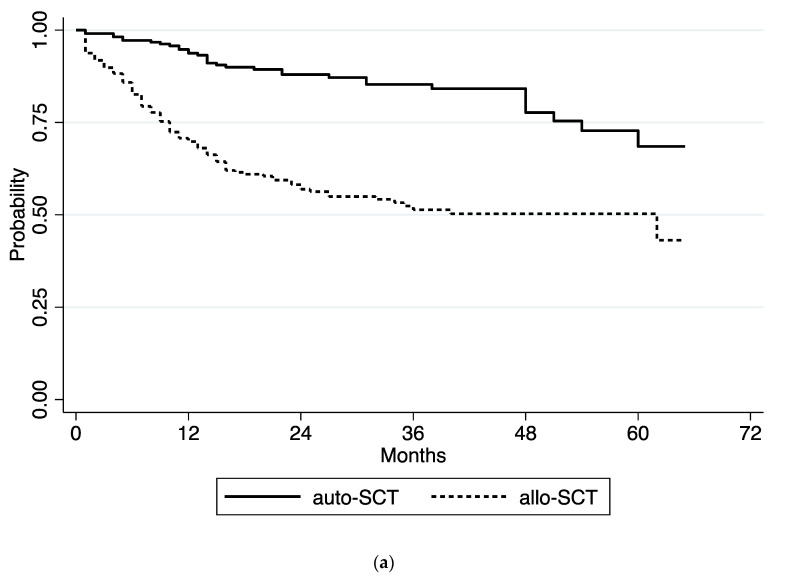
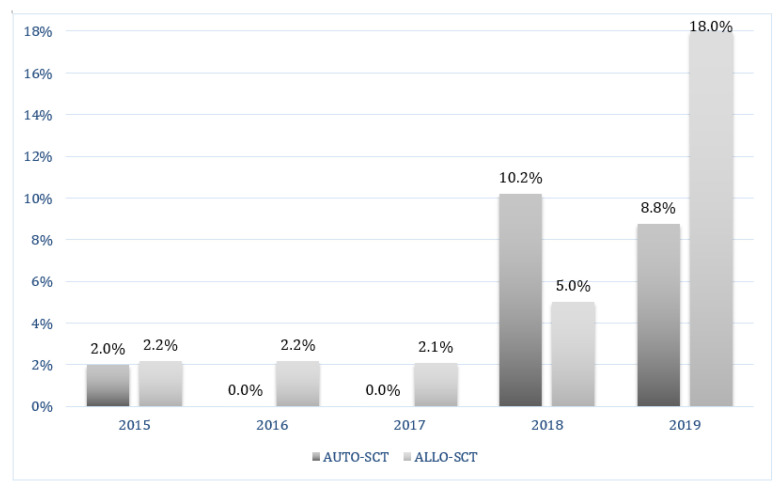
Patients who undergo hematopoietic stem cell transplants (HSCT) are at major risk of (CD) infection (CDI), the most common cause of nosocomial diarrhea. We conducted a retrospective study, which enrolled 481 patients who underwent autologous (220) or allogeneic HSCT (261) in a 5-year period, with the aim of identifying the incidence, risk factors and outcome of CDI between the start of conditioning and 100 days after HSCT. The overall cumulative incidence of CDI based upon clinical evidence was 5.4% (95% CI, 3.7% to 7.8%), without any significant difference between the two types of procedures. The median time between HSCT and CDI diagnosis was 12 days. Out of 26 patients, 19 (73%) with clinical and symptomatic evidence of CDI were positive also for enzymatic or molecular detection of toxigenic CD; in particular, in 5 out of 26 patients (19%) CD binary toxin was also detected. CDI diagnoses significantly increased in the period 2018-2019, since the introduction in the microbiology lab unit of the two-step diagnostic test based on GDH immunoenzymatic detection and toxin B/binary toxin/027 ribotype detection by real-time PCR. Via multivariate analysis, abdominal surgery within 10 years before HSCT ( = 0.002), antibiotic therapy within two months before HSCT ( = 0.000), HCV infection ( = 0.023) and occurrence of bacterial or fungal infections up to 100 days after HSCT ( = 0.003) were significantly associated with a higher risk of CDI development. The 26 patients were treated with first-line vancomycin (24) or fidaxomicine (2) and only 2 patients needed a second-line treatment, due to the persistence of stool positivity. No significant relationship was identified between CDI and the development of acute graft versus host disease (GVHD) after allogeneic HSCT. At a median follow-up of 25 months (range 1-65), the cumulative incidence of transplant related mortality (TRM) was 16.6% (95% CI 11.7% to 22.4%) and the 3-year overall survival (OS) was 67.0% (95% CI 61.9% to 71.6%). The development of CDI had no significant impact on TRM and OS, which were significantly impaired in the multivariate analysis by gastrointestinal and urogenital comorbidities, severe GVHD, previous infections or hospitalization within two months before HSCT, active disease at transplant and occurrence of infections after HSCT. We conclude that 20% of all episodes of diarrhea occurring up to 100 days after HSCT were related to toxigenic CD infection. Patients with a history of previous abdominal surgery or HCV infection, or those who had received broad spectrum parenteral antibacterial therapy were at major risk for CDI development. CDIs were successfully treated with vancomycin or fidaxomicin after auto-HSCT as well as after allo-HSCT.
接受造血干细胞移植(HSCT)的患者面临艰难梭菌(CD)感染(CDI)的重大风险,CDI是医院获得性腹泻最常见的病因。我们进行了一项回顾性研究,纳入了在5年期间接受自体(220例)或异基因HSCT(261例)的481例患者,目的是确定在预处理开始至HSCT后100天期间CDI的发病率、危险因素和结局。基于临床证据的CDI总体累积发病率为5.4%(95%CI,3.7%至7.8%),两种移植程序之间无显著差异。HSCT与CDI诊断之间的中位时间为12天。在26例患者中,19例(73%)有CDI的临床和症状证据,其产毒CD的酶学或分子检测也呈阳性;特别是,26例患者中有5例(19%)还检测到CD二元毒素。自微生物实验室引入基于GDH免疫酶检测和实时PCR检测毒素B/二元毒素/027核糖体分型的两步诊断试验以来,2018 - 2019年期间CDI诊断显著增加。通过多变量分析,HSCT前10年内的腹部手术(P = 0.002)、HSCT前两个月内的抗生素治疗(P = 0.000)、丙型肝炎病毒(HCV)感染(P = 0.023)以及HSCT后100天内发生的细菌或真菌感染(P = 0.003)与CDI发生风险较高显著相关。26例患者接受一线万古霉素(24例)或非达霉素(2例)治疗,仅2例患者因粪便持续阳性需要二线治疗。在异基因HSCT后,未发现CDI与急性移植物抗宿主病(GVHD)的发生之间存在显著关系。中位随访25个月(范围1 - 65个月)时,移植相关死亡率(TRM)的累积发病率为16.6%(95%CI 11.7%至22.4%),3年总生存率(OS)为67.0%(95%CI 61.9%至71.6%)。CDI的发生对TRM和OS无显著影响,在多变量分析中,胃肠道和泌尿生殖系统合并症、严重GVHD、HSCT前两个月内的既往感染或住院、移植时的活动性疾病以及HSCT后感染的发生会显著损害TRM和OS。我们得出结论,HSCT后100天内发生的所有腹泻发作中有20%与产毒CD感染有关。有既往腹部手术史或HCV感染史的患者,或接受过广谱胃肠外抗菌治疗的患者发生CDI的风险较高。自体HSCT以及异基因HSCT后,CDI用万古霉素或非达霉素成功治疗。