Department of Medicine, NYU Grossman School of Medicine, New York, New York.
Applied Bioinformatics Laboratories, NYU Grossman School of Medicine, New York, New York.
Clin Cancer Res. 2021 Jan 1;27(1):131-140. doi: 10.1158/1078-0432.CCR-20-2415. Epub 2020 Nov 18.
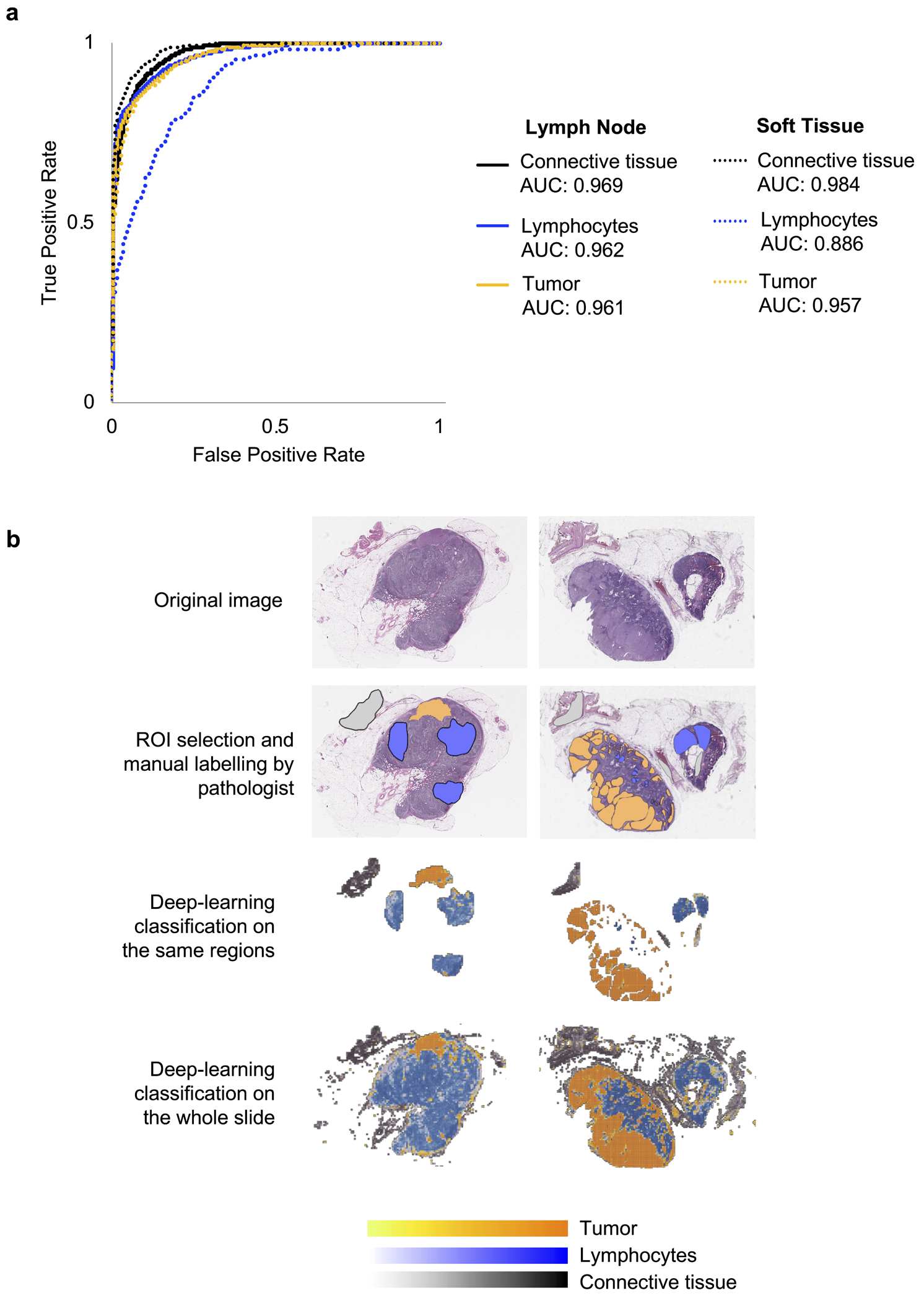
Several biomarkers of response to immune checkpoint inhibitors (ICI) show potential but are not yet scalable to the clinic. We developed a pipeline that integrates deep learning on histology specimens with clinical data to predict ICI response in advanced melanoma.
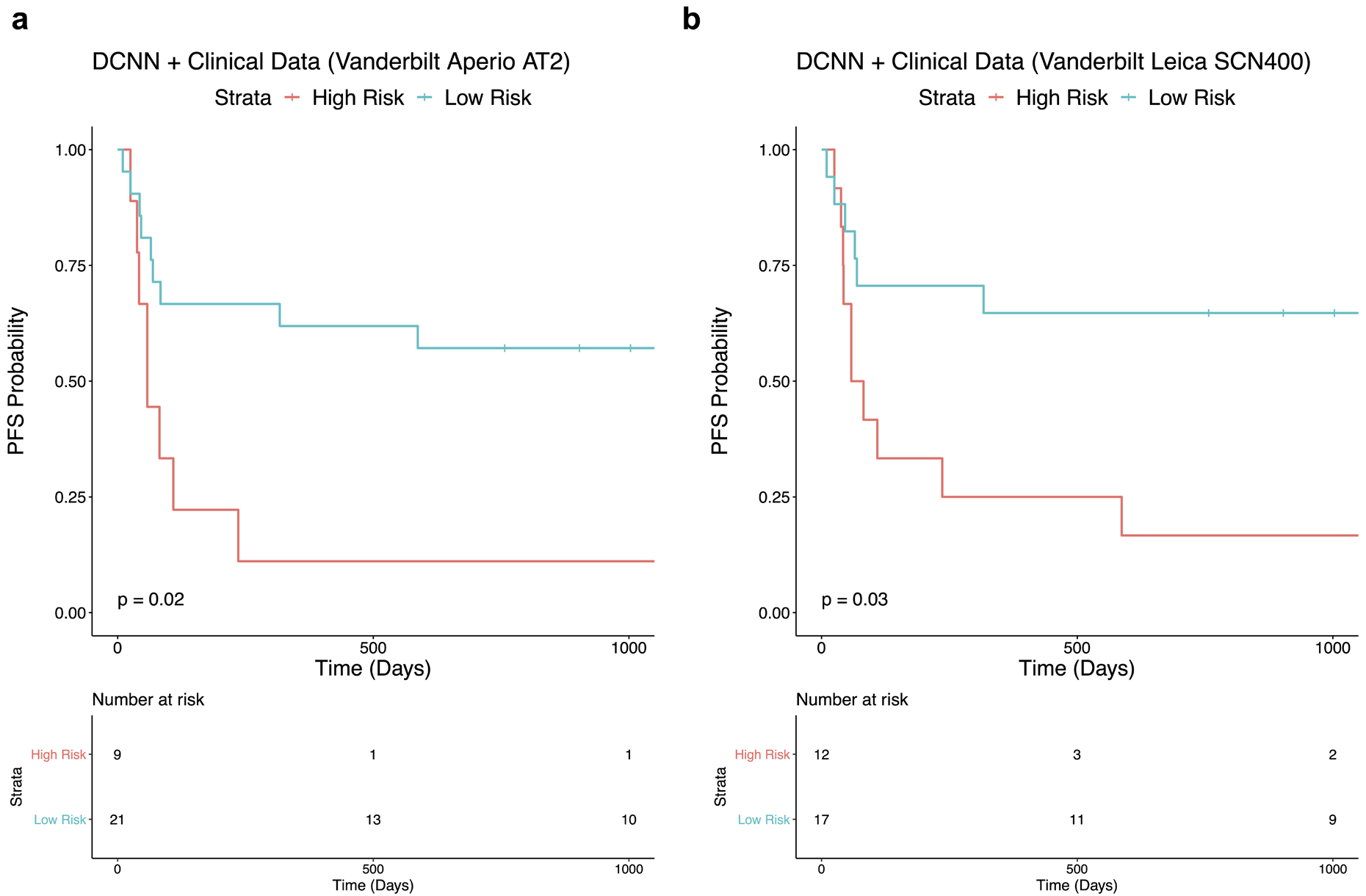
We used a training cohort from New York University (New York, NY) and a validation cohort from Vanderbilt University (Nashville, TN). We built a multivariable classifier that integrates neural network predictions with clinical data. A ROC curve was generated and the optimal threshold was used to stratify patients as high versus low risk for progression. Kaplan-Meier curves compared progression-free survival (PFS) between the groups. The classifier was validated on two slide scanners (Aperio AT2 and Leica SCN400).
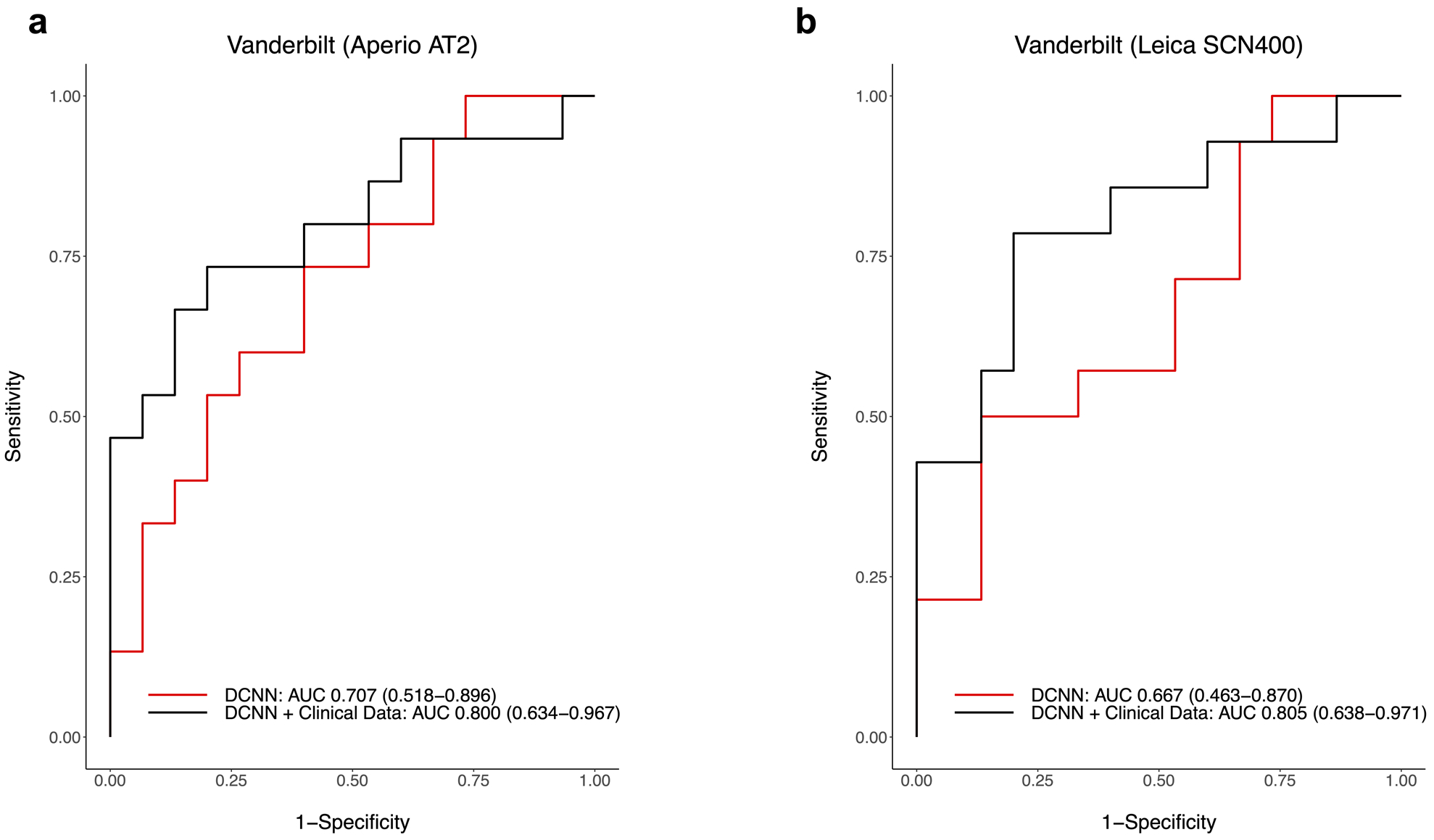
The multivariable classifier predicted response with AUC 0.800 on images from the Aperio AT2 and AUC 0.805 on images from the Leica SCN400. The classifier accurately stratified patients into high versus low risk for disease progression. Vanderbilt patients classified as high risk for progression had significantly worse PFS than those classified as low risk ( = 0.02 for the Aperio AT2; = 0.03 for the Leica SCN400).
Histology slides and patients' clinicodemographic characteristics are readily available through standard of care and have the potential to predict ICI treatment outcomes. With prospective validation, we believe our approach has potential for integration into clinical practice.
有几种免疫检查点抑制剂(ICI)反应的生物标志物显示出一定的潜力,但尚未推广到临床应用。我们开发了一个整合组织学标本深度学习与临床数据的管道,以预测晚期黑色素瘤对 ICI 的反应。
我们使用了来自纽约大学(纽约,NY)的训练队列和范德比尔特大学(纳什维尔,TN)的验证队列。我们构建了一个多变量分类器,将神经网络预测与临床数据相结合。生成了 ROC 曲线,并使用最佳阈值将患者分为进展高风险和低风险组。比较两组之间的无进展生存期(PFS)。该分类器在两个扫描仪(Aperio AT2 和 Leica SCN400)上进行了验证。
多变量分类器在 Aperio AT2 图像上的预测响应 AUC 为 0.800,在 Leica SCN400 图像上的 AUC 为 0.805。该分类器准确地将患者分为疾病进展的高风险和低风险组。被归类为进展高风险的范德比尔特患者的 PFS 明显差于被归类为低风险的患者(Aperio AT2 为 0.02;Leica SCN400 为 0.03)。
组织学切片和患者的临床病理特征通过标准护理很容易获得,并且有可能预测 ICI 治疗结果。通过前瞻性验证,我们相信我们的方法有可能整合到临床实践中。