Section of Hematology/Oncology, Department of Medicine, The University of Chicago, Chicago, Illinois.
Department of Radiation and Cellular Oncology, The University of Chicago, Chicago, Illinois.
JAMA Netw Open. 2020 Nov 2;3(11):e2025881. doi: 10.1001/jamanetworkopen.2020.25881.
Postoperative chemoradiation is the standard of care for cancers with positive margins or extracapsular extension, but the benefit of chemotherapy is unclear for patients with other intermediate risk features.
To evaluate whether machine learning models could identify patients with intermediate-risk head and neck squamous cell carcinoma who would benefit from chemoradiation.
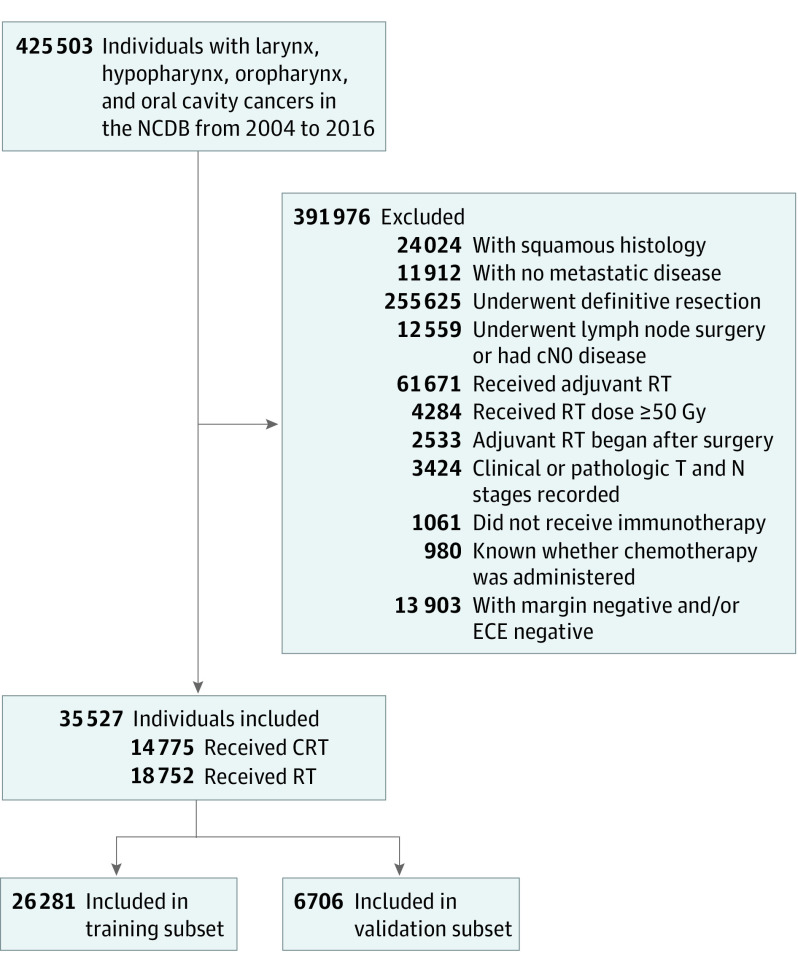
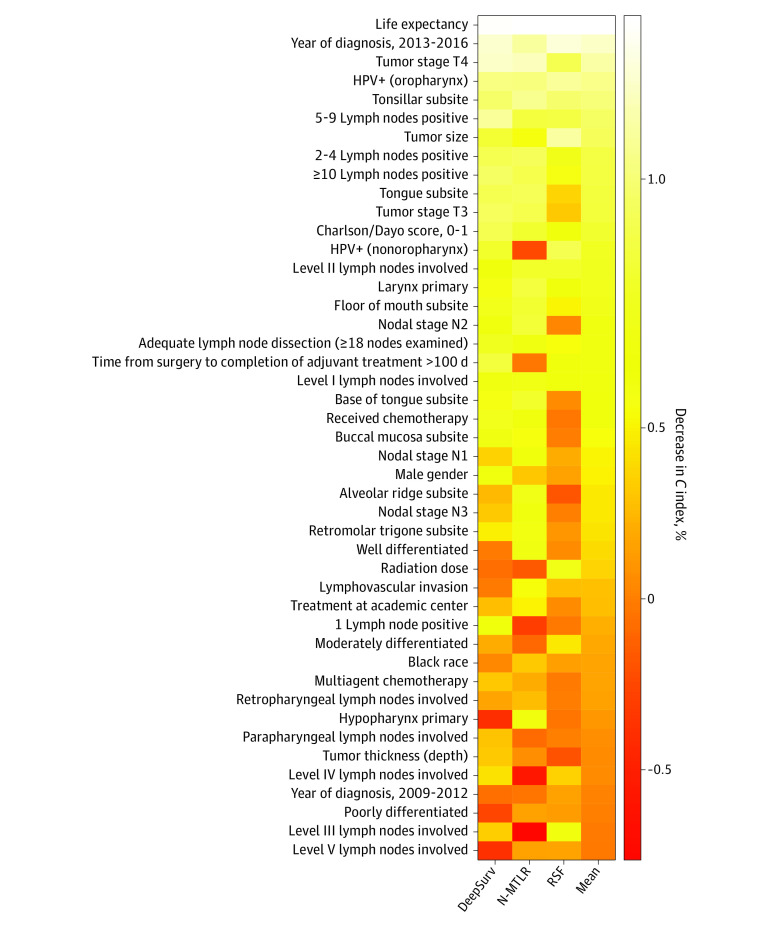
DESIGN, SETTING, AND PARTICIPANTS: This cohort study included patients diagnosed with squamous cell carcinoma of the oral cavity, oropharynx, hypopharynx, or larynx from January 1, 2004, through December 31, 2016. Patients had resected disease and underwent adjuvant radiotherapy. Analysis was performed from October 1, 2019, through September 1, 2020. Patients were selected from the National Cancer Database, a hospital-based registry that captures data from more than 70% of newly diagnosed cancers in the United States. Three machine learning survival models were trained using 80% of the cohort, with the remaining 20% used to assess model performance.
Receipt of adjuvant chemoradiation or radiation alone.
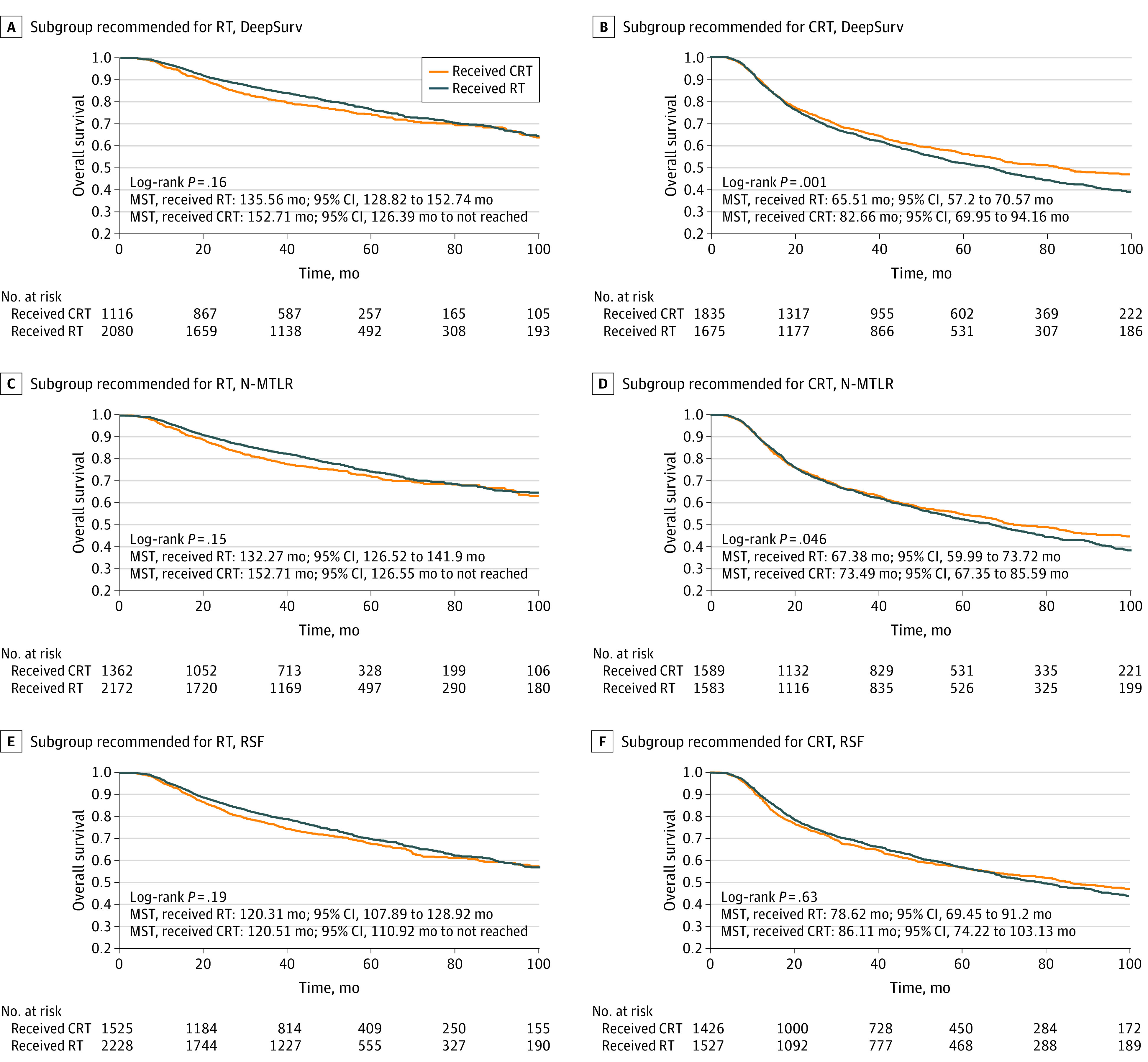
Patients who received treatment recommended by machine learning models were compared with those who did not. Overall survival for treatment according to model recommendations was the primary outcome. Secondary outcomes included frequency of recommendation for chemotherapy and chemotherapy benefit in patients recommended for chemoradiation vs radiation alone.
A total of 33 527 patients (24 189 [72%] men; 28 036 [84%] aged ≤70 years) met the inclusion criteria. Median follow-up in the validation data set was 43.2 (interquartile range, 19.8-65.5) months. DeepSurv, neural multitask logistic regression, and survival forest models recommended chemoradiation for 17 589 (52%), 15 917 (47%), and 14 912 patients (44%), respectively. Treatment according to model recommendations was associated with a survival benefit, with a hazard ratio of 0.79 (95% CI, 0.72-0.85; P < .001) for DeepSurv, 0.83 (95% CI, 0.77-0.90; P < .001) for neural multitask logistic regression, and 0.90 (95% CI, 0.83-0.98; P = .01) for random survival forest models. No survival benefit for chemotherapy was seen for patients recommended to receive radiotherapy alone.
These findings suggest that machine learning models may identify patients with intermediate risk who could benefit from chemoradiation. These models predicted that approximately half of such patients have no added benefit from chemotherapy.
术后放化疗是伴有阳性边缘或囊外扩展的癌症的标准治疗方法,但对于其他具有中等风险特征的患者,化疗的益处尚不清楚。
评估机器学习模型是否能够识别出具有中等风险的头颈部鳞状细胞癌患者,这些患者可能从放化疗中受益。
设计、设置和参与者:这项队列研究纳入了 2004 年 1 月 1 日至 2016 年 12 月 31 日期间被诊断为口腔、口咽、下咽或喉鳞状细胞癌的患者。患者患有经切除的疾病,并接受辅助放疗。分析于 2019 年 10 月 1 日至 2020 年 9 月 1 日进行。患者选自国家癌症数据库,这是一个基于医院的登记处,该数据库捕获了美国新诊断癌症的 70%以上的数据。使用队列的 80%来训练三个机器学习生存模型,其余 20%用于评估模型性能。
接受辅助放化疗或单纯放疗。
比较接受机器学习模型推荐治疗的患者与未接受治疗的患者。根据模型推荐的治疗的总生存率是主要结局。次要结局包括推荐化疗的频率以及在推荐放化疗与单纯放疗的患者中化疗的获益。
共有 33527 名患者(24189 名[72%]男性;28036 名[84%]年龄≤70 岁)符合纳入标准。验证数据集中的中位随访时间为 43.2(四分位距,19.8-65.5)个月。DeepSurv、神经多任务逻辑回归和生存森林模型分别建议对 17589 名(52%)、15917 名(47%)和 14912 名(44%)患者进行放化疗。根据模型推荐的治疗与生存获益相关,DeepSurv 的风险比为 0.79(95%CI,0.72-0.85;P<0.001),神经多任务逻辑回归的风险比为 0.83(95%CI,0.77-0.90;P<0.001),随机生存森林模型的风险比为 0.90(95%CI,0.83-0.98;P=0.01)。对于推荐接受单纯放疗的患者,化疗无生存获益。
这些发现表明,机器学习模型可能可以识别出具有中等风险且可能从放化疗中受益的患者。这些模型预测,大约一半的此类患者从化疗中没有额外获益。