Division of Cardiology, Department of Internal Medicine, Korea University Anam Hospital, Korea University School of Medicine, #73, Inchon-ro, Seongbuk-gu, Seoul, 02841, Korea.
Department of Cardiovascular Medicine, Regional Cardiocerebrovascular Center, Wonkwang University Medical Center, Iksan, Korea.
Sci Rep. 2020 Nov 19;10(1):20228. doi: 10.1038/s41598-020-77413-3.
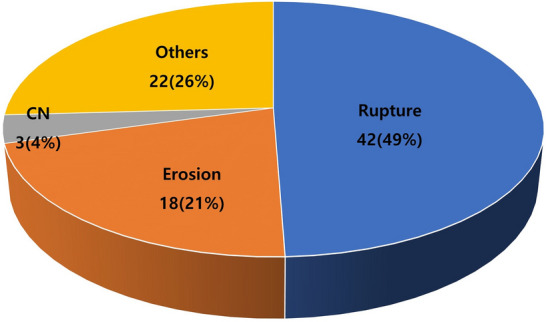
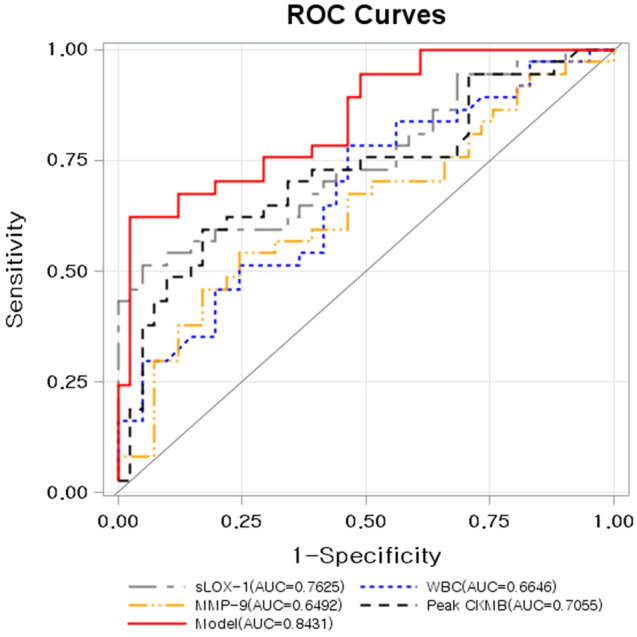
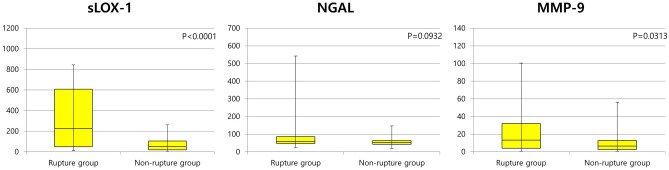
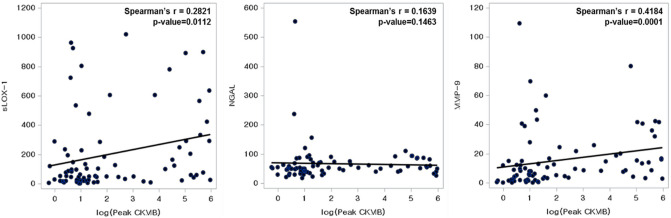
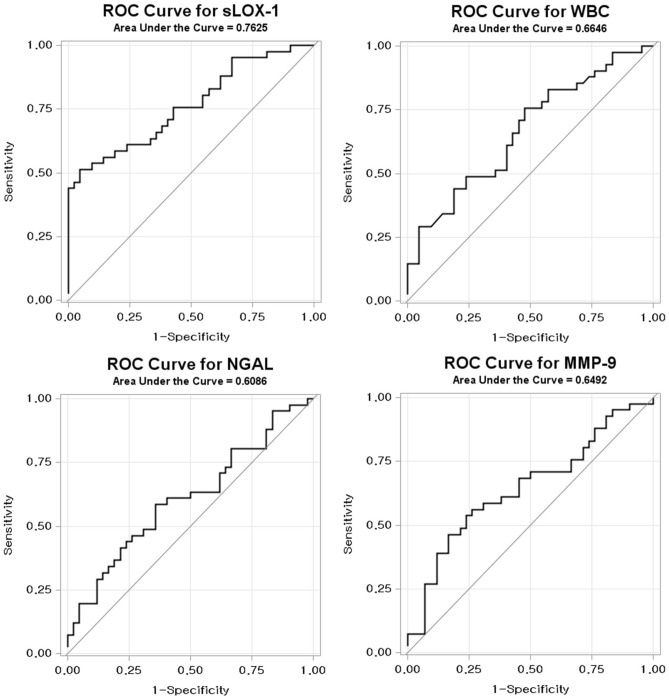
Soluble lectin-like oxidized low-density lipoprotein receptor-1 (sLOX-1), neutrophil gelatinase-associated lipocalin (NGAL), and matrix metalloproteinase-9 (MMP-9) are inflammatory biomarkers involved in plaque destabilization resulting in acute coronary syndrome (ACS). This study aimed to investigate the diagnostic value of a combination of biomarkers to discriminate plaque ruptures in the setting of ACS. Eighty-five ACS patients with optical coherence tomography (OCT) images of the culprit plaque were included and categorized into two groups: ACS with plaque rupture (Rupture group, n = 42) or without plaque rupture (Non-rupture group, n = 43) verified by OCT. A discriminative model of plaque rupture using several biomarkers was developed and validated. The Rupture group had higher white blood cell (WBC) counts and peak creatine kinase-myocardial band (CK-MB) levels (13.39 vs. 2.69 ng/mL, p = 0.0016). sLOX-1 (227.9 vs. 51.7 pg/mL, p < 0.0001) and MMP-9 (13.4 vs. 6.45 ng/mL, p = 0.0313) levels were significantly higher in the Rupture group, whereas NGAL showed a trend without statistical significance (59.03 vs. 53.80 ng/mL, p = 0.093). Receiver operating characteristic curves to differentiate Rupture group from Non-rupture group calculated the area under the curve for sLOX-1 (p < 0.001), MMP-9 (p = 0.0274), and NGAL (p = 0.0874) as 0.763, 0.645, and 0.609, respectively. A new combinatorial discriminative model including sLOX-1, MMP-9, WBC count, and the peak CK-MB level showed an area under the curve of 0.8431 (p < 0.001). With a cut-off point of 0.614, the sensitivity and specificity of plaque rupture were 62.2% and 97.6%, respectively. The new discriminative model using sLOX-1, MMP-9, WBC count, and peak CK-MB levels could better identify plaque rupture than each individual biomarker in ACS patients.
可溶性凝集素样氧化低密度脂蛋白受体-1(sLOX-1)、中性粒细胞明胶酶相关脂质运载蛋白(NGAL)和基质金属蛋白酶-9(MMP-9)是参与斑块不稳定导致急性冠脉综合征(ACS)的炎症生物标志物。本研究旨在探讨联合生物标志物诊断 ACS 患者斑块破裂的价值。共纳入 85 例接受光学相干断层扫描(OCT)检查的 ACS 患者,根据 OCT 结果将其分为斑块破裂组(破裂组,n=42)和非破裂组(非破裂组,n=43)。建立并验证了一种基于多种生物标志物的斑块破裂判别模型。破裂组的白细胞(WBC)计数和肌酸激酶同工酶-MB 峰值(CK-MB)水平更高(13.39 vs. 2.69ng/mL,p=0.0016)。sLOX-1(227.9 vs. 51.7pg/mL,p<0.0001)和 MMP-9(13.4 vs. 6.45ng/mL,p=0.0313)水平在破裂组中明显升高,而 NGAL 则无显著差异(59.03 vs. 53.80ng/mL,p=0.093)。计算区分破裂组和非破裂组的受试者工作特征曲线,sLOX-1(p<0.001)、MMP-9(p=0.0274)和 NGAL(p=0.0874)的曲线下面积分别为 0.763、0.645 和 0.609。包括 sLOX-1、MMP-9、WBC 计数和 CK-MB 峰值的新型组合判别模型的曲线下面积为 0.8431(p<0.001)。以 0.614 为截断点,斑块破裂的敏感性和特异性分别为 62.2%和 97.6%。与单一生物标志物相比,使用 sLOX-1、MMP-9、WBC 计数和 CK-MB 峰值的新型判别模型能更好地识别 ACS 患者的斑块破裂。