Department of Immunology, The Weizmann Institute of Science, Rehovot, Israel.
David H. Smith Center for Vaccine Biology and Immunology, Department of Microbiology and Immunology, University of Rochester Medical Center, Rochester, NY, USA.
Nat Rev Immunol. 2021 Jan;21(1):49-64. doi: 10.1038/s41577-020-00470-2. Epub 2020 Nov 19.
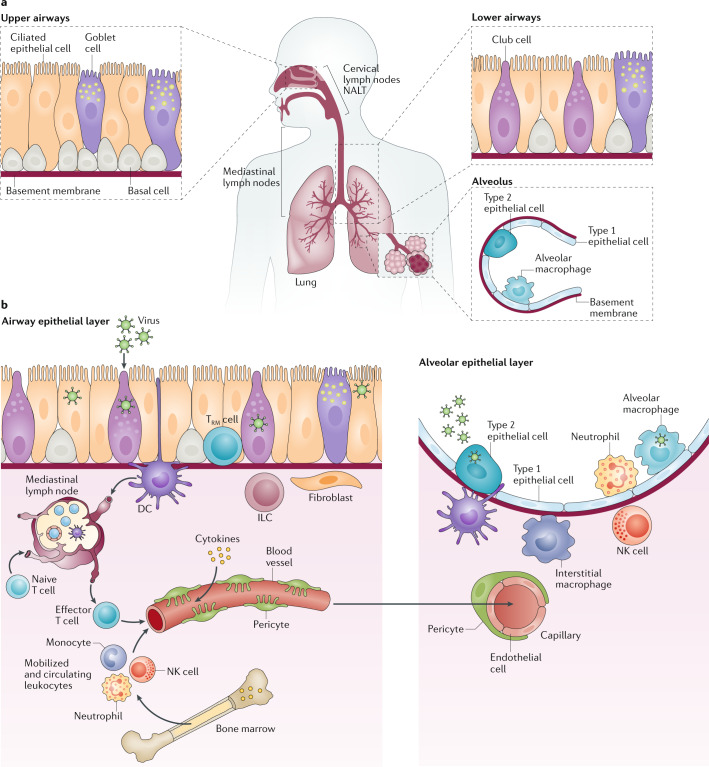
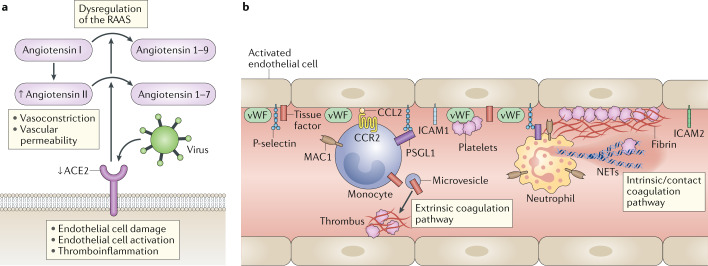
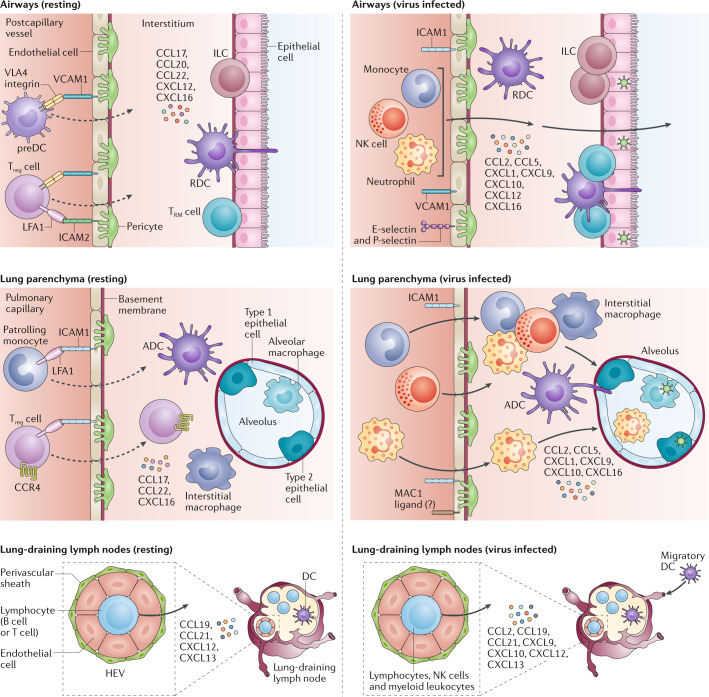
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the causative agent of coronavirus disease 2019 (COVID-19). Understanding of the fundamental processes underlying the versatile clinical manifestations of COVID-19 is incomplete without comprehension of how different immune cells are recruited to various compartments of virus-infected lungs, and how this recruitment differs among individuals with different levels of disease severity. As in other respiratory infections, leukocyte recruitment to the respiratory system in people with COVID-19 is orchestrated by specific leukocyte trafficking molecules, and when uncontrolled and excessive it results in various pathological complications, both in the lungs and in other organs. In the absence of experimental data from physiologically relevant animal models, our knowledge of the trafficking signals displayed by distinct vascular beds and epithelial cell layers in response to infection by SARS-CoV-2 is still incomplete. However, SARS-CoV-2 and influenza virus elicit partially conserved inflammatory responses in the different respiratory epithelial cells encountered early in infection and may trigger partially overlapping combinations of trafficking signals in nearby blood vessels. Here, we review the molecular signals orchestrating leukocyte trafficking to airway and lung compartments during primary pneumotropic influenza virus infections and discuss potential similarities to distinct courses of primary SARS-CoV-2 infections. We also discuss how an imbalance in vascular activation by leukocytes outside the airways and lungs may contribute to extrapulmonary inflammatory complications in subsets of patients with COVID-19. These multiple molecular pathways are potential targets for therapeutic interventions in patients with severe COVID-19.
严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)是 2019 年冠状病毒病(COVID-19)的病原体。如果不了解不同免疫细胞如何被招募到受病毒感染的肺部的不同部位,以及不同严重程度的个体之间这种招募有何不同,就无法完全理解 COVID-19 多变的临床表现的基本过程。与其他呼吸道感染一样,COVID-19 患者白细胞向呼吸系统的募集是由特定的白细胞迁移分子协调的,如果这种募集不受控制且过度,就会导致肺部和其他器官出现各种病理并发症。在缺乏来自生理相关动物模型的实验数据的情况下,我们对 SARS-CoV-2 感染后不同血管床和上皮细胞层显示的迁移信号的了解仍不完整。然而,SARS-CoV-2 和流感病毒在感染早期的不同呼吸道上皮细胞中引发部分保守的炎症反应,并可能在附近的血管中触发部分重叠的迁移信号组合。在这里,我们回顾了在原发性亲肺流感病毒感染期间协调白细胞向气道和肺区室迁移的分子信号,并讨论了与原发性 SARS-CoV-2 感染的不同病程的潜在相似性。我们还讨论了气道和肺外的白细胞对血管的激活失衡如何导致 COVID-19 患者亚群的肺外炎症并发症。这些多种分子途径是 COVID-19 重症患者治疗干预的潜在靶点。