Department of Ophthalmology, He Eye Specialists Hospitals, Shenyang, China.
Eye Hospital and School of Ophthalmology and Optometry, Wenzhou Medical University, Wenzhou, Zhejiang, China.
PLoS One. 2020 Nov 20;15(11):e0241630. doi: 10.1371/journal.pone.0241630. eCollection 2020.
To compare the accuracy of five kinds of intraocular lens calculation formulas (SRK/T, Haigis, Hoffer Q, Holladay and Barrett Universal Ⅱ) in cataract patients with steep curvature cornea ≥ 46.0 diopters.
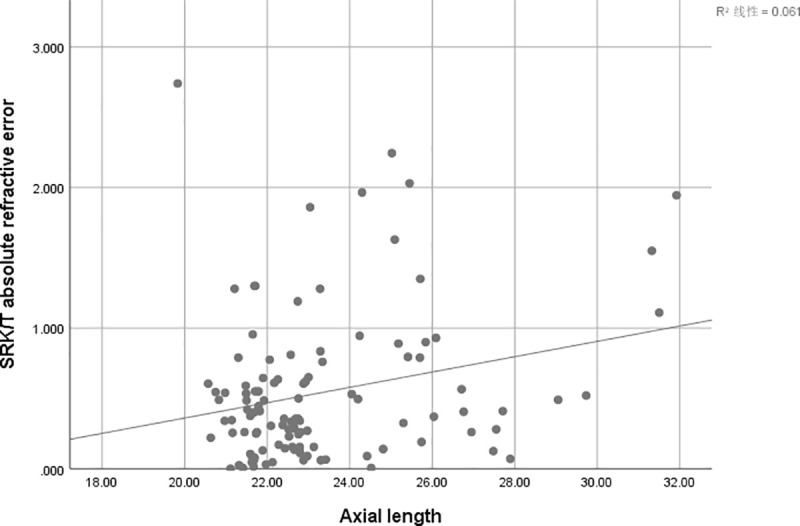
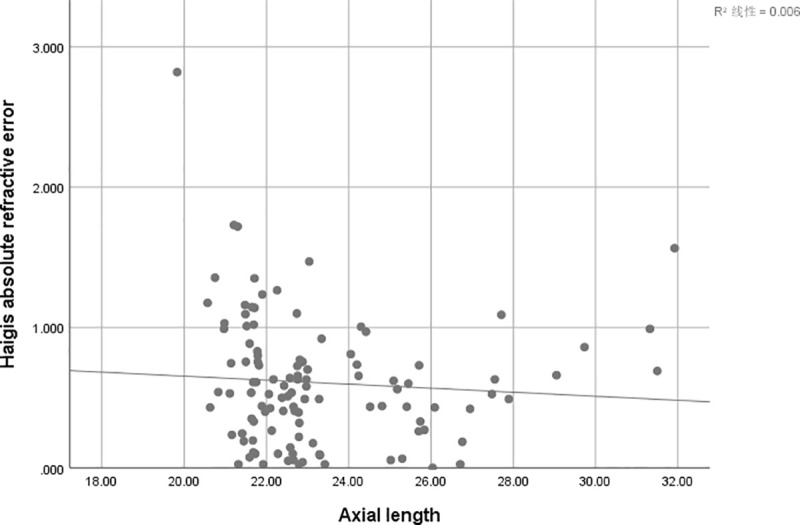
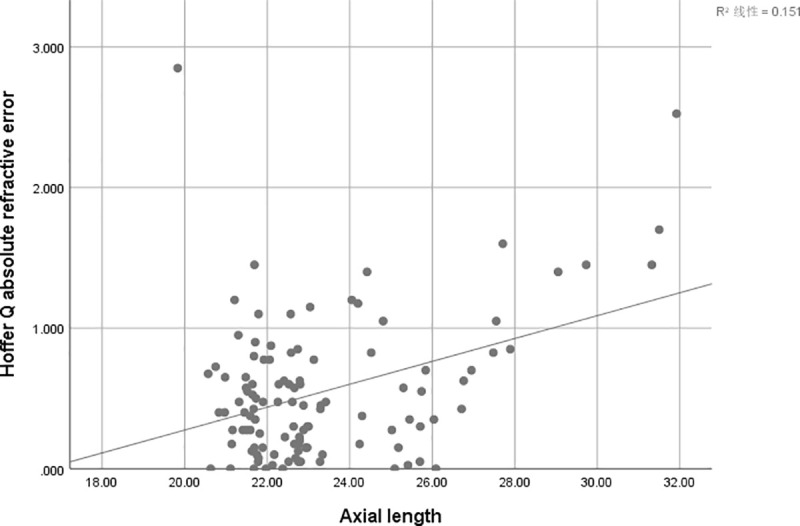
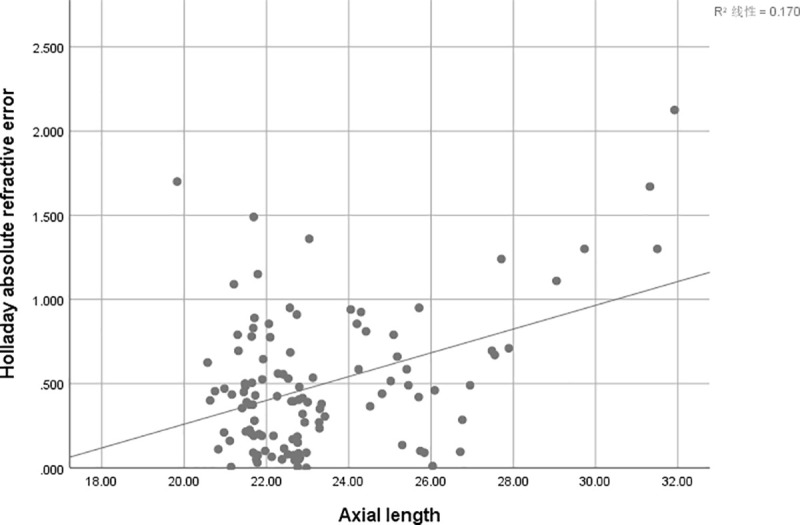
This is a retrospective study of cataract phacoemulsification combined with intraocular lens implantation in patients with steep curvature cornea (corneal curvature ≥ 46D). The refractive prediction errors of IOL power calculation formulas (SRK/T, Haigis, Holladay, Hoffer Q, and Barrett Universal II) using User Group for Laser Interference Biometry (ULIB) constants were evaluated and compared. Objective refraction results were assessed at one month postoperatively. According to axial length (AL), all patients were divided into three groups: short AL group (<22mm), normal AL group (>22 to ≤24.5mm) and long AL group (>24.5mm). Calculate the refractive error and absolute refractive error (AE) between the actual postoperative refractive power and the predicted postoperative refractive power. The covariance analysis was used for the comparison of five formulas in each group. The correlation between the absolute refractive error and AL from every formula were analyzed by Pearson correlation test, respectively.
Total 112 eyes of 83 cataract patients with steep curvature cornea were collected. The anterior chamber depth (ACD) was a covariate in the short AL group in the covariance analysis of absolute refractive error (P<0.001). The SRK/T and Holladay formula had the lowest mean absolute error (MAE) (0.47D), there were statistically significant differences in MAE between the five formulas for short AL group (P = 0.024). The anterior chamber depth had no significant correlation in the five calculation formulas in the normal AL group and long AL group (P = 0.521, P = 0.609 respectively). In the normal AL group, there was no significant difference in MAE between the five calculation formulas (P = 0.609). In the long AL group, Barrett Universal II formula had the lowest MAE (0.35), and there were statistically significant differences in MAE between the five formulas (P = 0.012). Over the entire AL range, the Barrett Universal II formula had the lowest MAE and the highest percentage of eyes within ± 0.50 D, ± 1.00 D, and ± 1.50 D (69.6%, 93.8%, and 98.2% respectively).
Compared to SRK/T, Haigis, Hoffer Q, and Holladay, Barrett Universal Ⅱ formula is more accurate in predicting the IOL power in the cataract patients with steep curvature cornea ≥ 46.0 diopters.
比较 5 种眼内晶状体计算公式(SRK/T、Haigis、Hoffer Q、Holladay 和 Barrett Universal Ⅱ)在角膜曲率≥46.0 屈光度的白内障患者中的准确性。
这是一项回顾性研究,纳入了角膜曲率(角膜曲率≥46D)较大的白内障患者行超声乳化白内障吸除联合人工晶状体植入术。使用用户组激光干涉生物测量(ULIB)常数评估并比较了眼内晶状体计算公式(SRK/T、Haigis、Holladay、Hoffer Q 和 Barrett Universal Ⅱ)的屈光预测误差。术后 1 个月评估客观屈光结果。根据眼轴(AL),所有患者分为三组:短 AL 组(<22mm)、正常 AL 组(>22 至≤24.5mm)和长 AL 组(>24.5mm)。计算实际术后屈光力与预测术后屈光力之间的屈光误差和绝对屈光误差(AE)。在每组中使用协方差分析比较五种公式。通过 Pearson 相关检验分别分析各公式的绝对屈光误差与 AL 的相关性。
共纳入 83 例角膜曲率较大的白内障患者的 112 只眼。在绝对屈光误差的协方差分析中,短 AL 组的前房深度(ACD)是一个协变量(P<0.001)。SRK/T 和 Holladay 公式的平均绝对误差(MAE)最低(0.47D),在短 AL 组的五种公式之间,MAE 有统计学差异(P=0.024)。在正常 AL 组和长 AL 组,前房深度与五种计算公式无显著相关性(P=0.521,P=0.609)。在正常 AL 组,五种计算公式的 MAE 无显著差异(P=0.609)。在长 AL 组,Barrett Universal II 公式的 MAE 最低(0.35),五种公式之间的 MAE 有统计学差异(P=0.012)。在整个 AL 范围内,Barrett Universal II 公式的 MAE 最低,有 69.6%、93.8%和 98.2%的眼在±0.50 D、±1.00 D 和±1.50 D范围内的比例最高。
与 SRK/T、Haigis、Hoffer Q 和 Holladay 相比,Barrett Universal Ⅱ 公式在预测角膜曲率≥46.0 屈光度的白内障患者的眼内晶状体屈光力方面更为准确。