Division of Endocrine and Oncologic Surgery, Department of Surgery, Tulane University, School of Medicine, New Orleans, LA, 70112, USA.
Division of Endocrine and Oncologic Surgery, Department of Surgery, Tulane University, School of Medicine, New Orleans, LA, 70112, USA; Genetics Unit, Department of Histology and Cell Biology, Faculty of Medicine, Suez Canal University, Ismailia, 41522, Egypt.
Respir Med. 2020 Dec;175:106205. doi: 10.1016/j.rmed.2020.106205. Epub 2020 Nov 11.
The novel coronavirus disease 2019 (COVID-19) has rapidly spread across the globe. Pre-existing comorbidities have been found to have a dramatic effect on the disease course. We sought to analyze the effect of asthma on the disease progression and outcomes of COVID-19 patients.
We conducted a multi-center retrospective study of positively confirmed COVID-19 patients. The primary outcome of interest was in-hospital mortality. Secondary outcomes were the Intensive Care Unit (ICU) admission, intubation, mechanical ventilation, and length of hospital stay.
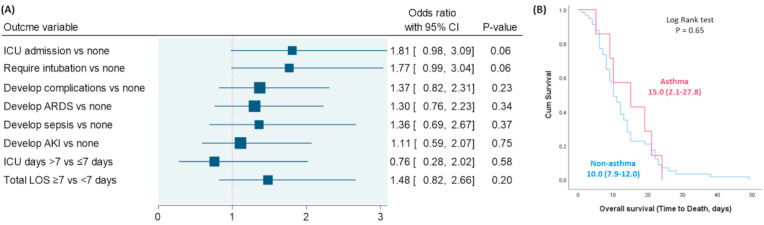
A total of 502 COVID-19 adult patients (72 asthma and 430 non-asthma cohorts) with mean age of 60.7 years were included in the study. The frequency of asthma in hospitalized cohorts was 14.3%. Univariate analysis revealed that asthma patients were more likely to be obese (75% versus 54.2%, p = 0.001), with a higher frequency of intubation (40.3% versus 27.8%, p = 0.036), and required a longer duration of hospitalization (15.1 ± 12.5 versus 11.5 ± 10.6, p = 0.015). After adjustment, multivariable analysis showed that asthmatic patients were not associated with higher risk of ICU admission (OR = 1.81, 95%CI = 0.98-3.09, p = 0.06), endotracheal intubation (OR = 1.77, 95%CI = 0.99-3.04, p = 0.06) or complications (OR = 1.37, 95%CI = 0.82-2.31, p = 0.23). Asthmatic patients were not associated with higher odds of prolonged hospital length of stay (OR = 1.48, 95%CI = 0.82-2.66, p = 0.20) or with ICU stay (OR = 0.76, 95%CI = 0.28-2.02, p = 0.58). Kaplan-Meier curve showed no significant difference in the overall survival of the two groups (p = 0.65).
Despite the increased prevalence of hospitalization in elder asthmatic COVID-19 patients, after adjustment for other variables, it was neither associated with increased severity nor worse outcomes.
2019 年新型冠状病毒病(COVID-19)在全球迅速蔓延。已经发现先前存在的合并症对疾病进程有显著影响。我们旨在分析哮喘对 COVID-19 患者疾病进展和结局的影响。
我们对确诊的 COVID-19 成年患者进行了一项多中心回顾性研究。主要观察终点为住院死亡率。次要结局为重症监护病房(ICU)入住、插管、机械通气和住院时间。
共纳入 502 例 COVID-19 成年患者(72 例哮喘和 430 例非哮喘队列),平均年龄 60.7 岁。住院患者中哮喘的频率为 14.3%。单因素分析显示,哮喘患者更易肥胖(75%比 54.2%,p=0.001),插管的频率更高(40.3%比 27.8%,p=0.036),住院时间更长(15.1±12.5 比 11.5±10.6,p=0.015)。校正后多变量分析显示,哮喘患者入住 ICU 的风险无显著增加(OR=1.81,95%CI=0.98-3.09,p=0.06)、气管插管(OR=1.77,95%CI=0.99-3.04,p=0.06)或并发症(OR=1.37,95%CI=0.82-2.31,p=0.23)的风险无显著增加。哮喘患者的住院时间延长(OR=1.48,95%CI=0.82-2.66,p=0.20)或 ICU 入住(OR=0.76,95%CI=0.28-2.02,p=0.58)的可能性无显著增加。Kaplan-Meier 曲线显示两组的总体生存率无显著差异(p=0.65)。
尽管老年哮喘 COVID-19 患者住院率增加,但在调整其他变量后,与疾病严重程度或结局恶化无关。