Department of Neurology and Clinical Neuroscience Center, University Hospital Zurich and University of Zurich, Zurich, Switzerland.
Epidemiology, Biostatistics and Prevention Institute (EBPI), University of Zurich, Zurich, Switzerland.
Eur J Neurol. 2021 Apr;28(4):1234-1243. doi: 10.1111/ene.14651. Epub 2020 Dec 21.
Clinical outcomes vary substantially among individuals with large vessel occlusion (LVO) stroke. A small infarct core and large imaging mismatch were found to be associated with good recovery. The aim of this study was to investigate whether those imaging variables would improve individual prediction of functional outcome after early (<6 h) endovascular treatment (EVT) in LVO stroke.
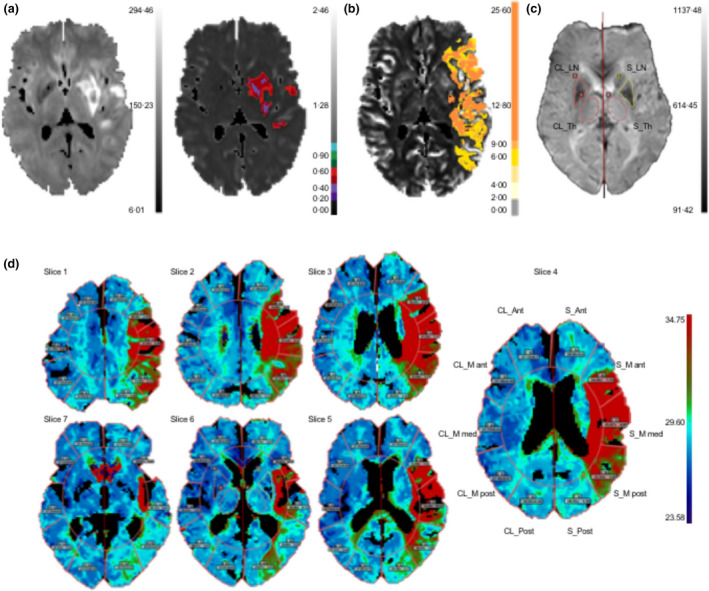
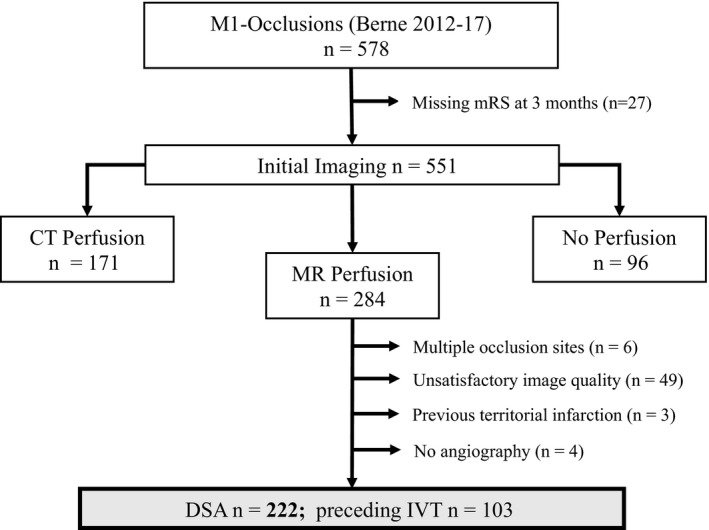
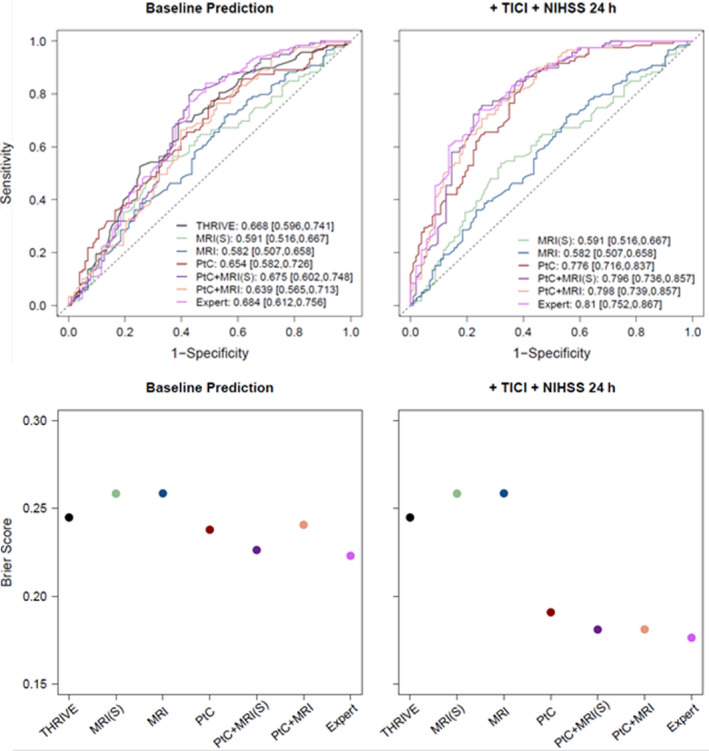
We included 222 patients with acute ischemic stroke due to middle cerebral artery (MCA)-M1 occlusion who received EVT. As predictors, we used clinical variables and region of interest (ROI)-based magnetic resonance imaging features. We developed different machine-learning models and quantified their prediction performance according to the area under the receiver-operating characteristic curves and the Brier score.
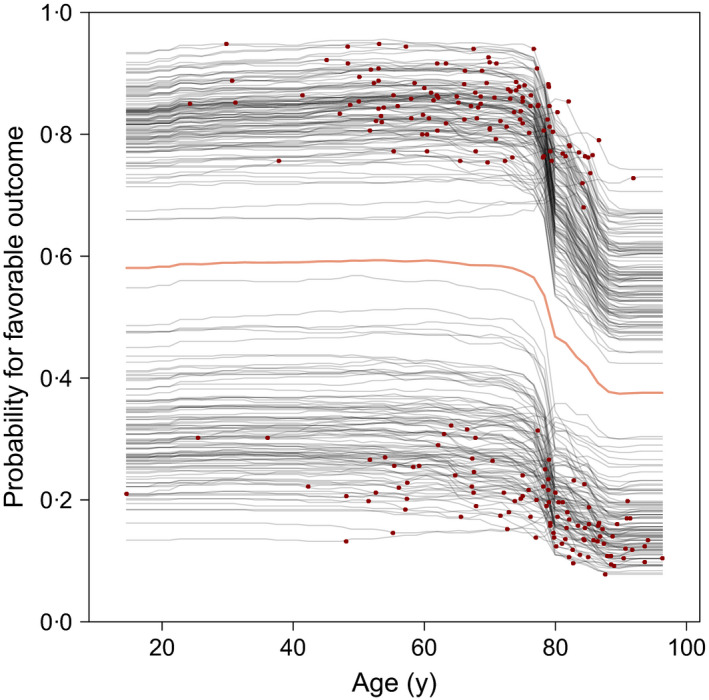
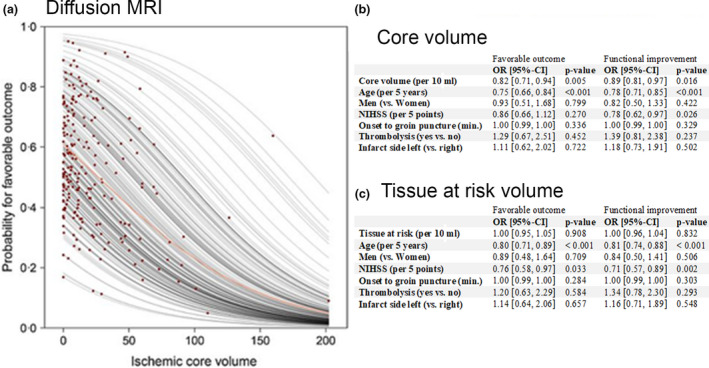
The rate of successful recanalization was 78%, with 54% patients having a favorable outcome (modified Rankin scale score 0-2). Small infarct core was associated with favorable functional outcome. Outcome prediction improved only slightly when imaging was added to patient variables. Age was the driving factor, with a sharp decrease in likelihood of favorable functional outcome above the age of 78 years.
In patients with MCA-M1 occlusion strokes referred to EVT within 6 h of symptom onset, infarct core volume was associated with outcome. However, ROI-based imaging variables led to no significant improvement in outcome prediction at an individual patient level when added to a set of clinical predictors. Our study is in concordance with current practice, where imaging mismatch or collateral readouts are not recommended as factors for excluding patients with MCA-M1 occlusion for early EVT.
大血管闭塞(LVO)卒中患者的临床结局存在很大差异。小梗死核心和大影像不匹配与良好的恢复相关。本研究旨在探讨这些影像变量是否能改善 LVO 卒中患者早期(<6 小时)血管内治疗(EVT)后功能结局的个体预测。
我们纳入了 222 例因大脑中动脉(MCA)M1 闭塞导致的急性缺血性卒中患者,他们接受了 EVT。作为预测因素,我们使用了临床变量和基于感兴趣区域(ROI)的磁共振成像特征。我们开发了不同的机器学习模型,并根据接收者操作特征曲线下面积和 Brier 评分来量化它们的预测性能。
再通成功率为 78%,54%的患者预后良好(改良 Rankin 量表评分 0-2)。小梗死核心与良好的功能结局相关。当将影像学结果加入到患者变量中时,预后预测仅略有改善。年龄是一个驱动因素,超过 78 岁时,预后良好的可能性急剧下降。
在症状发作后 6 小时内接受 EVT 的 MCA-M1 闭塞卒中患者中,梗死核心体积与结局相关。然而,当加入一组临床预测因子时,基于 ROI 的影像学变量对个体患者的结局预测没有显著改善。我们的研究与当前的实践一致,即不建议将影像不匹配或侧支循环读数作为排除 MCA-M1 闭塞患者早期 EVT 的因素。