Mutke Matthias A, Madai Vince I, Hilbert Adam, Zihni Esra, Potreck Arne, Weyland Charlotte S, Möhlenbruch Markus A, Heiland Sabine, Ringleb Peter A, Nagel Simon, Bendszus Martin, Frey Dietmar
Department of Neuroradiology, Heidelberg University Hospital, Heidelberg, Germany.
Charité Lab for Artificial Intelligence in Medicine, Charité Universitätsmedizin Berlin, Berlin, Germany.
Front Neurol. 2022 May 27;13:737667. doi: 10.3389/fneur.2022.737667. eCollection 2022.
Outcome prediction after mechanical thrombectomy (MT) in patients with acute ischemic stroke (AIS) and large vessel occlusion (LVO) is commonly performed by focusing on favorable outcome (modified Rankin Scale, mRS 0-2) after 3 months but poor outcome representing severe disability and mortality (mRS 5 and 6) might be of equal importance for clinical decision-making.
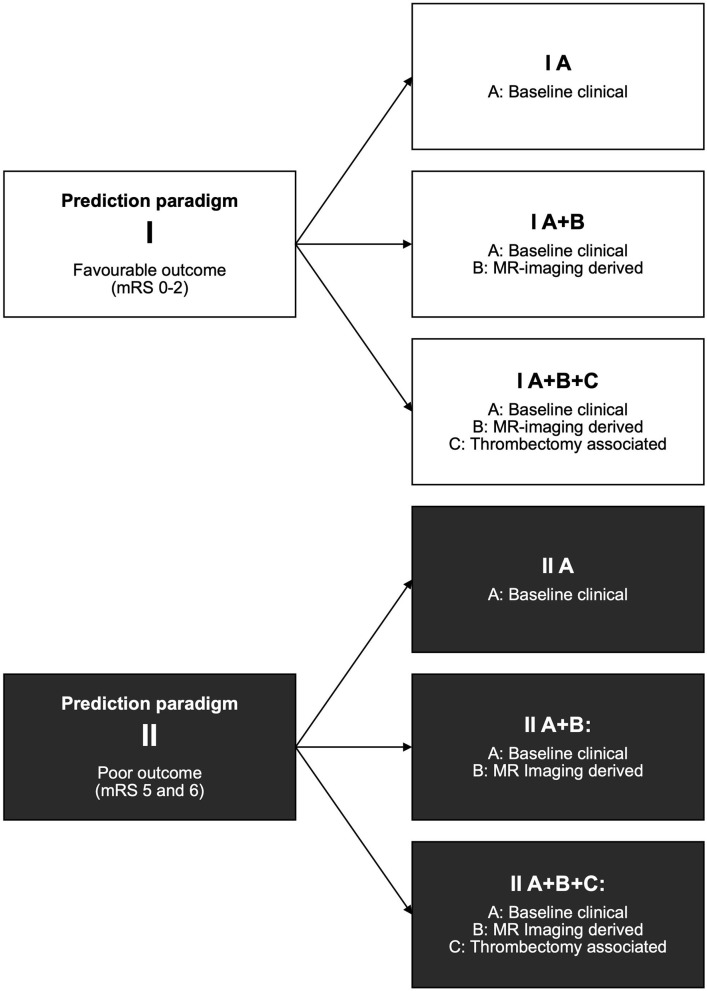
We retrospectively analyzed patients with AIS and LVO undergoing MT from 2009 to 2018. Prognostic variables were grouped in baseline clinical (A), MRI-derived variables including mismatch [apparent diffusion coefficient (ADC) and time-to-maximum (Tmax) lesion volume] (B), and variables reflecting speed and extent of reperfusion (C) [modified treatment in cerebral ischemia (mTICI) score and time from onset to mTICI]. Three different scenarios were analyzed: (1) baseline clinical parameters only, (2) baseline clinical and MRI-derived parameters, and (3) all baseline clinical, imaging-derived, and reperfusion-associated parameters. For each scenario, we assessed prediction for favorable and poor outcome with seven different machine learning algorithms.
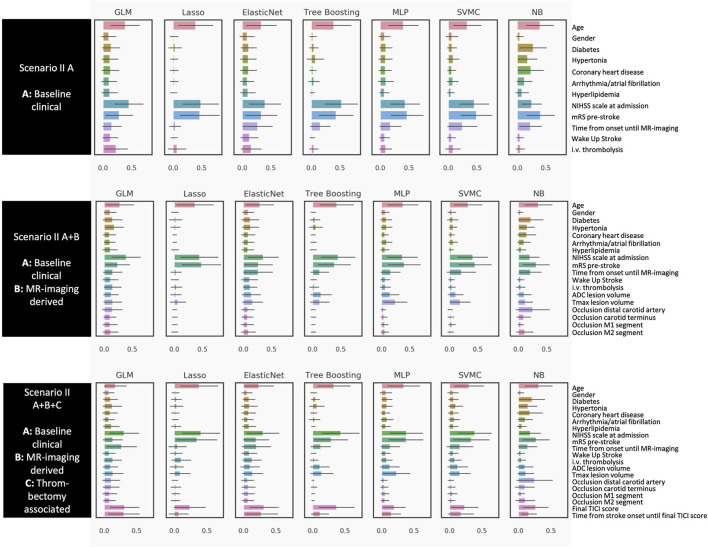
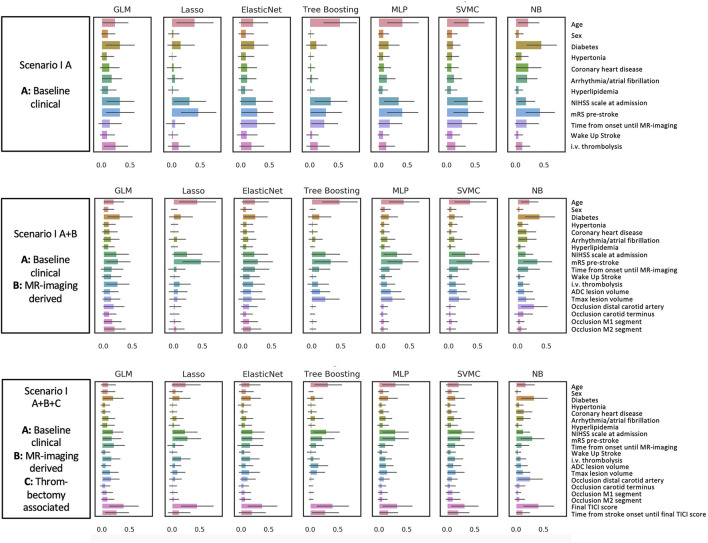
In 210 patients, prediction of favorable outcome was improved after including speed and extent of recanalization [highest area under the curve (AUC) 0.73] compared to using baseline clinical variables only (highest AUC 0.67). Prediction of poor outcome remained stable by using baseline clinical variables only (highest AUC 0.71) and did not improve further by additional variables. Prediction of favorable and poor outcomes was not improved by adding MR-mismatch variables. Most important baseline clinical variables for both outcomes were age, National Institutes of Health Stroke Scale, and premorbid mRS.
Our results suggest that a prediction of poor outcome after AIS and MT could be made based on clinical baseline variables only. Speed and extent of MT did improve prediction for a favorable outcome but is not relevant for poor outcome. An MR mismatch with small ischemic core and larger penumbral tissue showed no predictive importance.
急性缺血性卒中(AIS)合并大血管闭塞(LVO)患者接受机械取栓治疗(MT)后的预后预测通常聚焦于3个月后的良好预后(改良Rankin量表,mRS 0 - 2),但代表严重残疾和死亡的不良预后(mRS 5和6)对于临床决策可能同样重要。
我们回顾性分析了2009年至2018年接受MT治疗的AIS合并LVO患者。将预后变量分为基线临床变量(A)、MRI衍生变量(包括不匹配[表观扩散系数(ADC)和最大强化时间(Tmax)病变体积])(B)以及反映再灌注速度和程度的变量(C)[脑缺血改良治疗(mTICI)评分和从发病到mTICI的时间]。分析了三种不同情况:(1)仅基线临床参数,(2)基线临床和MRI衍生参数,(3)所有基线临床、影像衍生和再灌注相关参数。对于每种情况,我们使用七种不同的机器学习算法评估对良好和不良预后的预测。
在210例患者中,与仅使用基线临床变量相比,纳入再通速度和程度后,良好预后的预测得到改善[曲线下面积(AUC)最高为0.73](仅使用基线临床变量时AUC最高为0.67)。仅使用基线临床变量时,不良预后的预测保持稳定(AUC最高为0.71),增加其他变量后并未进一步改善。添加MR不匹配变量后,良好和不良预后的预测均未改善。两种预后最重要的基线临床变量是年龄、美国国立卫生研究院卒中量表评分和病前mRS。
我们的结果表明,仅基于临床基线变量就可以对AIS和MT后的不良预后进行预测。MT的速度和程度确实改善了对良好预后的预测,但与不良预后无关。小缺血核心和较大半暗带组织的MR不匹配没有显示出预测重要性。