St Jeor Jeffery D, Jackson Taylor J, Xiong Ashley E, Freedman Brett A, Sebastian Arjun S, Currier Bradford L, Fogelson Jeremy L, Bydon Mohamad, Nassr Ahmad, Elder Benjamin D
Mayo Clinic School of Medicine, Rochester, MN, USA.
Department of Orthopedic Surgery, Mayo Clinic, Rochester, MN, USA.
Global Spine J. 2022 Jun;12(5):851-857. doi: 10.1177/2192568220975365. Epub 2020 Nov 23.
Retrospective Study.
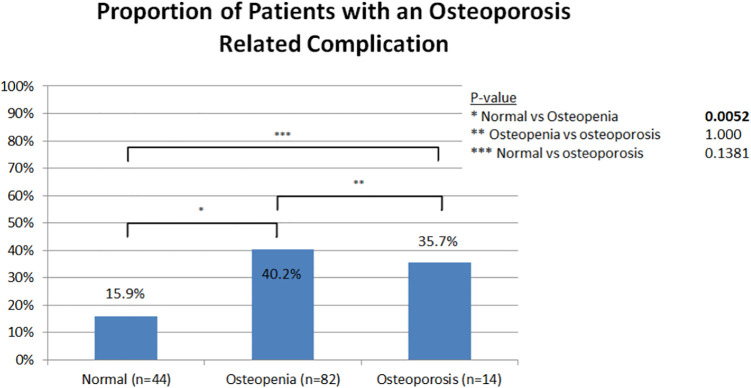
To compare methods of assessing pre-operative bone density to predict risk for osteoporosis related complications (ORC), defined as proximal junctional kyphosis, pseudarthrosis, accelerated adjacent segment disease, reoperation, compression fracture, and instrument failure following spine fusions.
Chart review of primary posterior thoracolumbar or lumbar fusion patients during a 7 year period. Inclusion criteria: preoperative dual-energy x-ray absorptiometry (DXA) test within 1 year and lumbar CT scan within 6 months prior to surgery with minimum of 1 year follow-up. Exclusion criteria: <18 years at time of index procedure, infection, trauma, malignancy, skeletal dysplasia, neuromuscular disorders, or anterior-posterior procedures.
140 patients were included. The average age was 67.9 years, 83 (59.3%) were female, and 45 (32%) had an ORC. There were no significant differences in patient characteristics between those with and without an ORC. Multilevel fusions were associated with ORCs (46.7% vs 26.3%, p = 0.02). Patients with ORCs had lower DXA t-scores (-1.62 vs -1.10, p = 0.003) and average Hounsfield units (HU) (112.1 vs 148.1, p ≤ 0.001). Multivariable binary logistic regression analysis showed lower average HU (Adj. OR 0.00 595% CI 0.0001-0.1713, p = 0.001) was an independent predictor of an ORC. The odds of an ORC increased by 1.7-fold for every 25 point decrease in average HU.
The gold standard for assessing bone mineral density has been DXA t-scores, but the best predictor of ORC remains unclear. While both lower t-scores and average HU were associated with ORC, only HU was an independent predictor of ORC.
回顾性研究。
比较术前评估骨密度的方法,以预测骨质疏松相关并发症(ORC)的风险,ORC定义为脊柱融合术后近端交界性后凸、假关节形成、相邻节段疾病加速进展、再次手术、压缩性骨折和内固定失败。
对7年间接受初次后路胸腰段或腰椎融合术的患者进行病历回顾。纳入标准:术前1年内进行双能X线吸收法(DXA)检测,术前6个月内进行腰椎CT扫描,且至少随访1年。排除标准:初次手术时年龄<18岁、感染、创伤、恶性肿瘤、骨骼发育异常、神经肌肉疾病或前后路联合手术。
共纳入140例患者。平均年龄为67.9岁,83例(59.3%)为女性,45例(32%)发生ORC。发生ORC和未发生ORC的患者在特征上无显著差异。多节段融合与ORC相关(46.7%对26.3%,p = 0.02)。发生ORC的患者DXA t值较低(-1.62对-1.10,p = 0.003),平均亨氏单位(HU)也较低(112.1对148.1,p≤0.001)。多变量二元逻辑回归分析显示,较低的平均HU(调整后比值比0.00,95%置信区间0.0001 - 0.1713,p = 0.001)是ORC的独立预测因素。平均HU每降低25分,ORC的发生几率增加1.7倍。
评估骨矿物质密度的金标准一直是DXA t值,但ORC的最佳预测因素仍不明确。虽然较低的t值和平均HU均与ORC相关,但只有HU是ORC的独立预测因素。