Bogossian Elisa G, Taccone Fabio S, Izzi Antonio, Yin Nicolas, Garufi Alessandra, Hublet Stephane, Njimi Hassane, Ego Amedee, Gorham Julie, Byl Baudouin, Brasseur Alexandre, Hites Maya, Vincent Jean-Louis, Creteur Jacques, Grimaldi David
Department of Intensive Care, CUB-Hôpital Erasme, Université Libre de Bruxelles, 1070 Brussels, Belgium.
Department of Microbiology, LHUB-ULB, Université Libre de Bruxelles, 1070 Brussels, Belgium.
Microorganisms. 2020 Nov 19;8(11):1821. doi: 10.3390/microorganisms8111821.
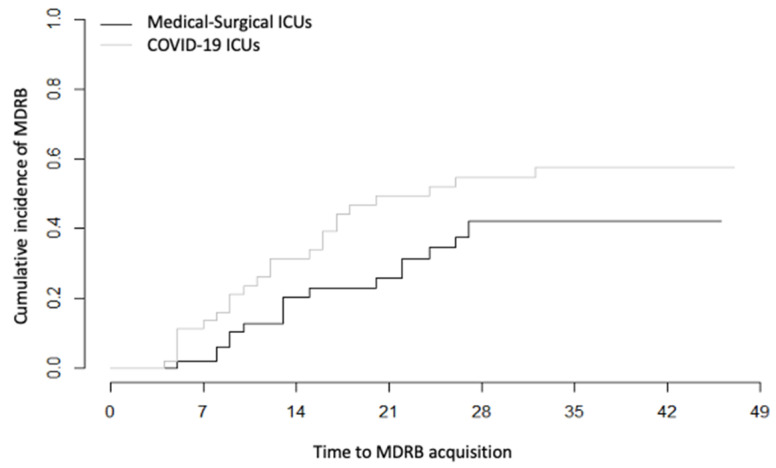
Whether the risk of multidrug-resistant bacteria (MDRB) acquisition in the intensive care unit (ICU) is modified by the COVID-19 crisis is unknown. In this single center case control study, we measured the rate of MDRB acquisition in patients admitted in COVID-19 ICU and compared it with patients admitted in the same ICU for subarachnoid hemorrhage (controls) matched 1:1 on length of ICU stay and mechanical ventilation. All patients were systematically and repeatedly screened for MDRB carriage. We compared the rate of MDRB acquisition in COVID-19 patients and in control using a competing risk analysis. Of note, although we tried to match COVID-19 patients with septic shock patients, we were unable due to the longer stay of COVID-19 patients. Among 72 patients admitted to the COVID-19 ICUs, 33% acquired 31 MDRB during ICU stay. The incidence density of MDRB acquisition was 30/1000 patient days. Antimicrobial therapy and exposure time were associated with higher rate of MDRB acquisition. Among the 72 SAH patients, 21% acquired MDRB, with an incidence density was 18/1000 patient days. The septic patients had more comorbidities and a greater number of previous hospitalizations than the COVID-19 patients. The incidence density of MDRB acquisition was 30/1000 patient days. The association between COVID-19 and MDRB acquisition (compared to control) risk did not reach statistical significance in the multivariable competing risk analysis (sHR 1.71 (CI 95% 0.93-3.21)). Thus, we conclude that, despite strong physical isolation, acquisition rate of MDRB in ICU patients was at least similar during the COVID-19 first wave compared to previous period.
重症监护病房(ICU)中获得多重耐药菌(MDRB)的风险是否会因新冠疫情危机而改变尚不清楚。在这项单中心病例对照研究中,我们测量了入住新冠ICU患者的MDRB获得率,并将其与因蛛网膜下腔出血入住同一ICU的患者(对照组)进行比较,两组在ICU住院时间和机械通气方面按1:1匹配。所有患者均被系统且反复地筛查MDRB携带情况。我们使用竞争风险分析比较了新冠患者和对照组中MDRB的获得率。值得注意的是,尽管我们试图将新冠患者与感染性休克患者进行匹配,但由于新冠患者住院时间较长而未能成功。在72名入住新冠ICU的患者中,33%在ICU住院期间获得了31种MDRB。MDRB获得的发病密度为每1000患者日30例。抗菌治疗和暴露时间与更高的MDRB获得率相关。在72名蛛网膜下腔出血患者中,21%获得了MDRB,发病密度为每1000患者日18例。感染性休克患者比新冠患者有更多的合并症和更多的既往住院史。MDRB获得的发病密度为每1000患者日30例。在多变量竞争风险分析中,新冠与MDRB获得(与对照组相比)风险之间的关联未达到统计学显著性(sHR 1.71(95%CI 0.93 - 3.