Kang Min-Seok, Hwang Jin-Ho, Choi Dae-Jung, Chung Hoon-Jae, Lee Jong-Hwa, Kim Hyong-Nyun, Park Hyun-Jin
Department of Orthopedic Surgery, Bumin Hospital, Seoul, Republic of Korea.
Department of Orthopedic Surgery, Himnaera Hospital, Busan, Republic of Korea.
J Orthop Surg Res. 2020 Nov 23;15(1):557. doi: 10.1186/s13018-020-02087-6.
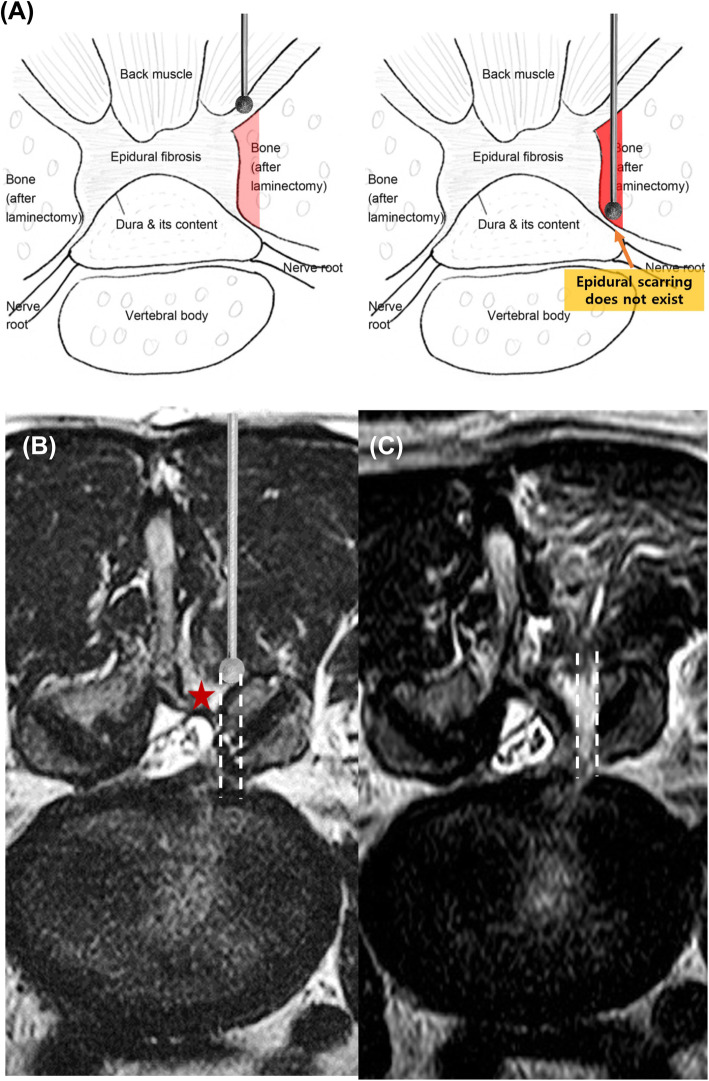
Although literature provides evidence regarding the superiority of surgery over conservative treatment in patients with lumbar disc herniation, recurrent lumbar disc herniation (RLDH) was the indication for reoperation in 62% of the cases. The major problem with revisional lumbar discectomy (RLD) is that the epidural scar tissue is not clearly isolated from the boundaries of the dura matter and nerve roots; therefore, unintended durotomy and nerve root injury may occur. The biportal endoscopic (BE) technique is a newly emerging minimally invasive spine surgical modality. However, clinical evidence regarding BE-RLD remains limited. We aimed to compare the clinical outcomes after performing open microscopic (OM)-RLD and BE-RLD to evaluate the feasibility of BE-RLD.
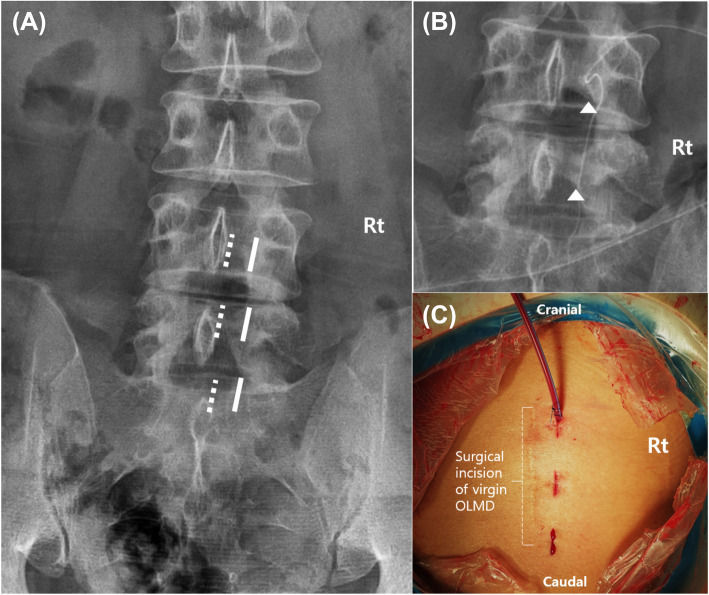
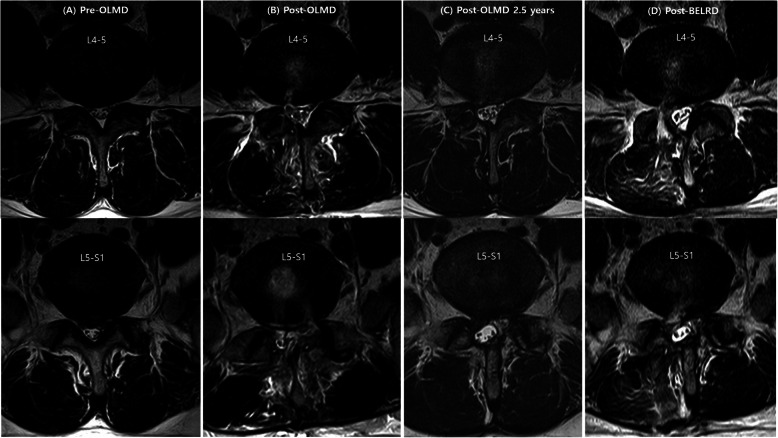
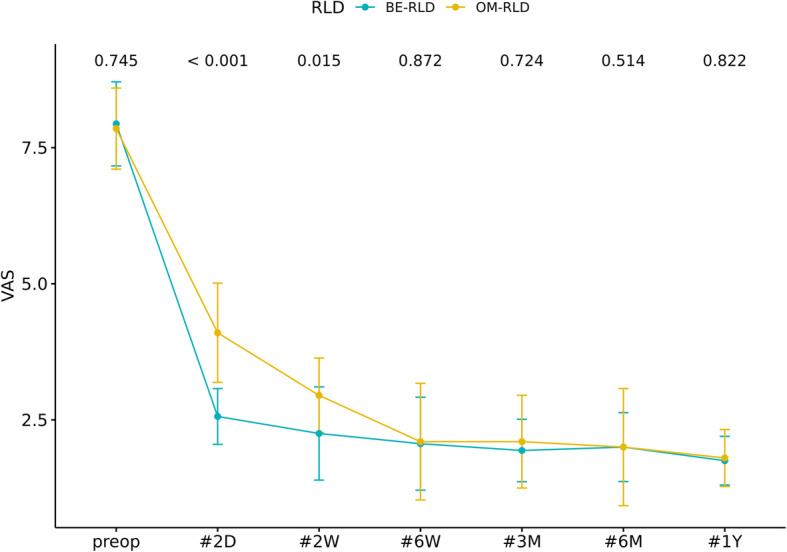
This retrospective study included 36 patients who were diagnosed with RLDH and underwent OM-RLD and BE-RLD. RLDH is defined as the presence of herniated disc material at the level previously operated upon in patients who have experienced a pain-free phase for more than 6 months. BE-RLD was performed as follows: two independent surgical ports were made inside the medial pedicular line of the target segment and on the intact upper and lower laminas. Peeling off the soft tissue from the vertebral lamina helps to easily identify the traversing nerve root and the recurrent disc material without dealing with the fibrotic scar tissue. Clinical outcomes were obtained using a visual analog scale (VAS) and the modified Macnab criteria before and at 2 days, 2 and 6 weeks, and 3, 6, and 12 months after surgery.
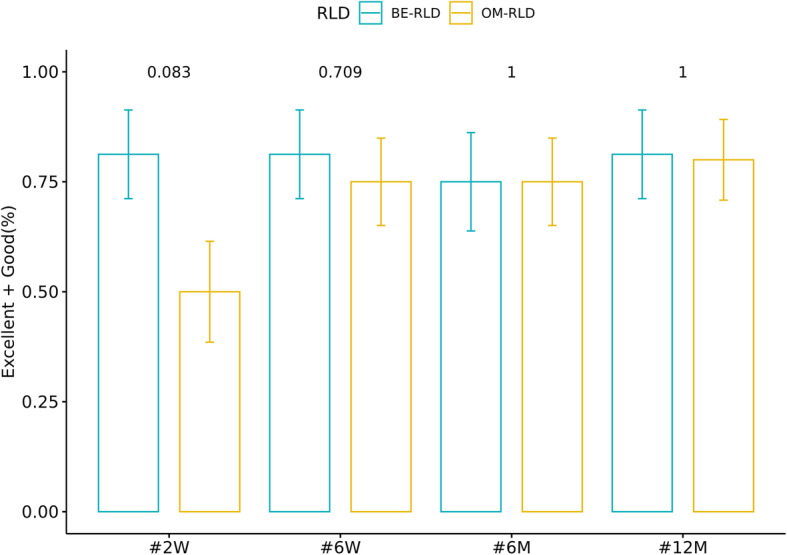
The data of 20 and 16 patients who underwent OM-RLD and BE-RLD, respectively, were evaluated. The demographic and perioperative data were comparable between the groups. During the year following the surgery, in the BE-RLD group, the VAS scores at each point were significantly improved over the baseline and remained improved up to 2 weeks after surgery (p < 0.05); however, no statistical difference between the two groups was observed after 6 weeks of surgery (p > 0.05). According to the modified Macnab criteria on the follow-up, the excellent or good satisfaction rates reported at 2 weeks, 6 weeks, 6 months, and 12 months after surgery were 81.25%, 81.25%, 75%, and 81.25%, respectively, in the BE-RLD group, and 50%, 75%, 75%, and 80%, respectively, in the OM-RLD group.
BE-RLD yielded similar outcomes to OM-RLD, including pain improvement, functional improvement, and patient satisfaction, at 1 year after surgery. However, faster pain relief, earlier functional recovery, and better patient satisfaction were observed when applying BE-LRD.
Retrospectively registered.
尽管文献表明在腰椎间盘突出症患者中手术优于保守治疗,但复发性腰椎间盘突出症(RLDH)是62%病例再次手术的指征。翻修性腰椎间盘切除术(RLD)的主要问题是硬膜外瘢痕组织与硬脊膜和神经根边界无法清晰分离;因此,可能会意外切开硬脊膜和损伤神经根。双门内镜(BE)技术是一种新兴的微创脊柱手术方式。然而,关于BE-RLD的临床证据仍然有限。我们旨在比较开放性显微镜下(OM)-RLD和BE-RLD后的临床结果,以评估BE-RLD的可行性。
这项回顾性研究纳入了36例被诊断为RLDH并接受OM-RLD和BE-RLD的患者。RLDH定义为在经历超过6个月无痛期的患者中,在先前手术节段存在椎间盘突出物质。BE-RLD的操作如下:在目标节段内侧椎弓根线内以及完整的上下椎板上制作两个独立的手术切口。从椎板上剥离软组织有助于轻松识别横过的神经根和复发性椎间盘物质,而无需处理纤维化瘢痕组织。在手术前以及术后2天、2周和6周、3个月、6个月和12个月,使用视觉模拟量表(VAS)和改良Macnab标准获得临床结果。
分别对20例接受OM-RLD和16例接受BE-RLD患者的数据进行了评估。两组的人口统计学和围手术期数据具有可比性。在手术后的一年中,在BE-RLD组,各时间点的VAS评分均较基线显著改善,且在术后2周内一直保持改善(p < 0.05);然而,术后6周两组之间未观察到统计学差异(p > 0.05)。根据随访时的改良Macnab标准,BE-RLD组在术后2周、6周、6个月和12个月报告的优良满意度分别为81.25%、81.25%、75%和81.25%,OM-RLD组分别为50%、75%、75%和80%。
术后1年时,BE-RLD在疼痛改善、功能改善和患者满意度方面产生了与OM-RLD相似的结果。然而,应用BE-LRD时观察到疼痛缓解更快、功能恢复更早且患者满意度更高。
回顾性注册。