Gstoettner Clemens, Laengle Gregor, Salminger Stefan, Festin Christopher, Platzgummer Hannes, Aszmann Oskar C
Klinisches Labor für Bionische Extremitätenrekonstruktion, Universitätsklinik für Chirurgie, Medizinische Universität Wien, Währinger Gürtel 18-20, 1090, Wien, Österreich.
Klinische Abteilung für Plastische und Rekonstruktive Chirurgie, Universitätsklinik für Chirurgie, Medizinische Universität Wien, Wien, Österreich.
Orthopade. 2021 Jan;50(1):14-23. doi: 10.1007/s00132-020-04032-1.
After limb loss, it is the surgeon's task to provide the patient with a pain-free and resilient residual limb. Particularly in the upper extremity, there is an additional functional aspect, as appropriate muscle signals are needed to control myoelectric prostheses. Surgical management of peripheral nerves within the residual limb plays a central role both in terms of pain treatment as well as functional human-machine interfacing.
The presentation of current surgical procedures for dealing with peripheral nerves after limb amputation.
A literature search is carried out regarding the surgical prophylaxis and therapy of neuroma and phantom limb pain, as well as techniques to improve the functional interface between residual limb and prosthesis. Practical recommendations are formulated based on relevant literature, as well as the experiences of the authors.
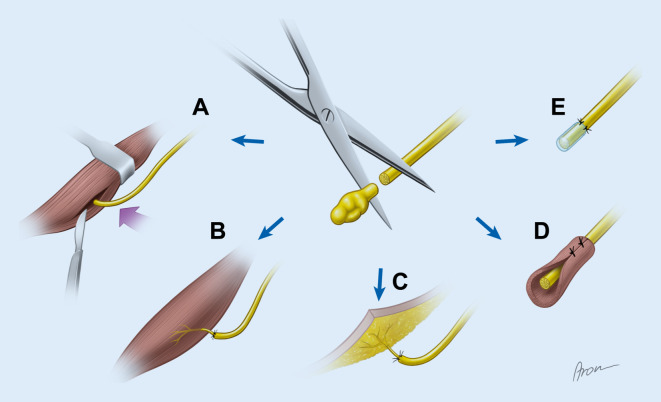
There is a large number of different surgical techniques, particularly for the management of painful neuromas. Of the conventional methods, intramuscular implantation of the terminal nerves is commonly used with good results. Newer techniques such as targeted muscle reinnervation (TMR) and the regenerative peripheral nerve interface (RPNI) aim for the first time to provide functional end organs to the nerve even after amputation. In addition to the improved control of myoelectric prostheses, these methods further show excellent results for treatment and prevention of neuroma and phantom limb pain.
肢体缺失后,外科医生的任务是为患者提供无痛且有弹性的残肢。特别是在上肢,还有一个额外的功能方面,因为需要适当的肌肉信号来控制肌电假肢。残肢内周围神经的外科处理在疼痛治疗以及功能性人机接口方面都起着核心作用。
介绍肢体截肢后处理周围神经的当前外科手术方法。
对神经瘤和幻肢痛的外科预防和治疗以及改善残肢与假肢之间功能接口的技术进行文献检索。根据相关文献以及作者的经验制定实用建议。
有大量不同的外科技术,特别是用于处理疼痛性神经瘤。在传统方法中,终末神经肌肉内植入术常用且效果良好。诸如靶向肌肉再支配(TMR)和再生周围神经接口(RPNI)等新技术首次旨在即使在截肢后也为神经提供功能性终末器官。除了改善肌电假肢的控制外,这些方法在治疗和预防神经瘤及幻肢痛方面也显示出优异的效果。