Wolfson Centre for Personalised Medicine, University of Liverpool, Liverpool, L69 3GL, UK.
Franciscus Gasthuis & Vlietland, Rotterdam, the Netherlands.
BMC Med. 2020 Nov 25;18(1):367. doi: 10.1186/s12916-020-01827-z.
The number of patients living with co-existing diseases is growing. This study aimed to assess the extent of multimorbidity, medication use, and drug- and gene-based interactions in patients following a non-ST elevation acute coronary syndrome (NSTE-ACS).
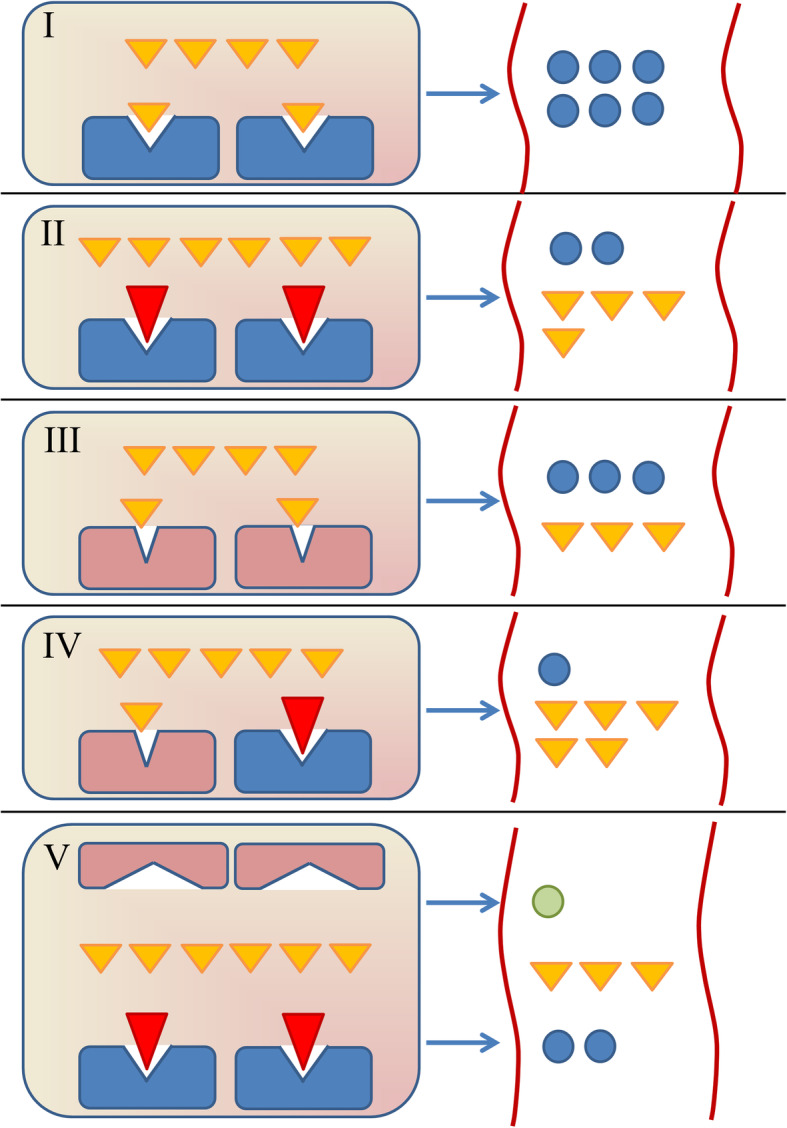
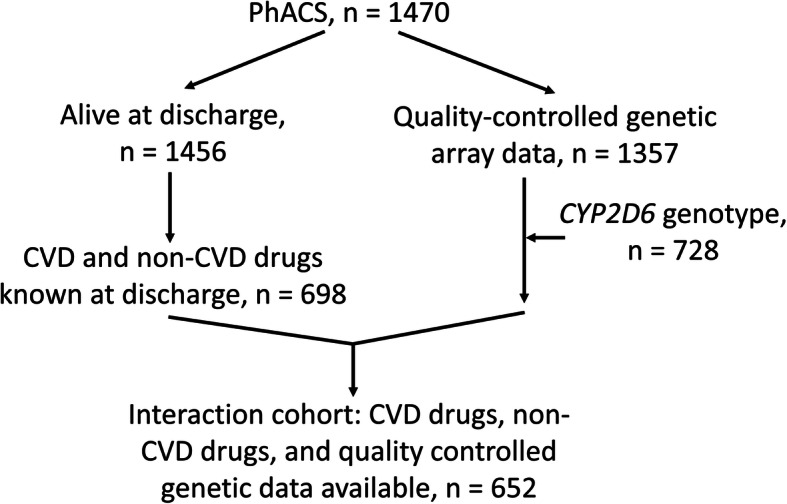
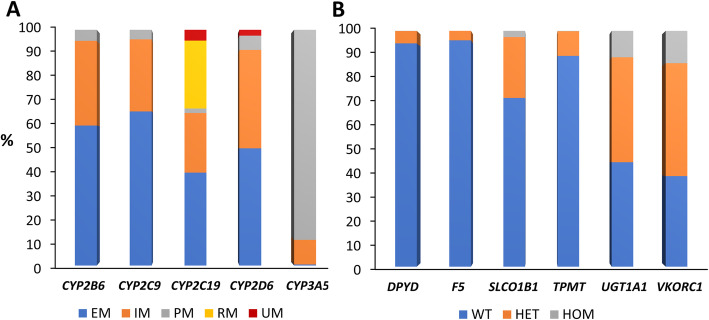
In 1456 patients discharged from hospital for a NSTE-ACS, comorbidities and multimorbidity (≥ 2 chronic conditions) were assessed. Of these, 698 had complete drug use recorded at discharge, and 652 (the 'interaction' cohort) had drug use and actionable genotypes available for CYP2B6, CYP2C9, CYP2C19, CYP2D6, CYP3A5, DPYD, F5, SLCO1B1, TPMT, UGT1A1, and VKORC1. The following drug interactions were investigated: pharmacokinetic drug-drug (DDIs) involving CYPs (CYPs above, plus CYP1A2, CYP2C8, CYP3A4), SLCO1B1, and P-glycoprotein; drug-gene (DGIs); drug-drug-gene (DDGIs); and drug-gene-gene (DGGIs). Interactions predicted to be 'substantial' were defined as follows: DDIs due to strong inhibitors/inducers, DGIs due to variant homozygous/compound heterozygous genotypes, and DDGIs/DGGIs where the constituent DDI/DGI(s) both influenced the victim drug in the same direction.
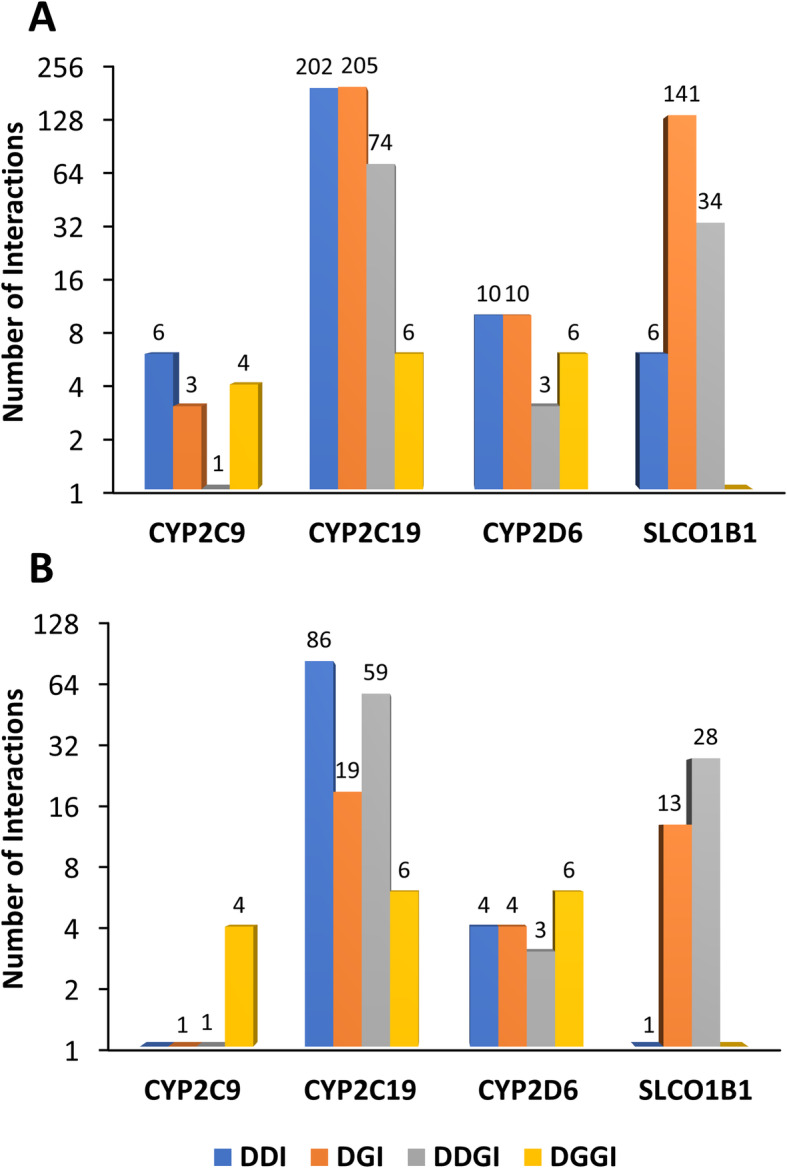
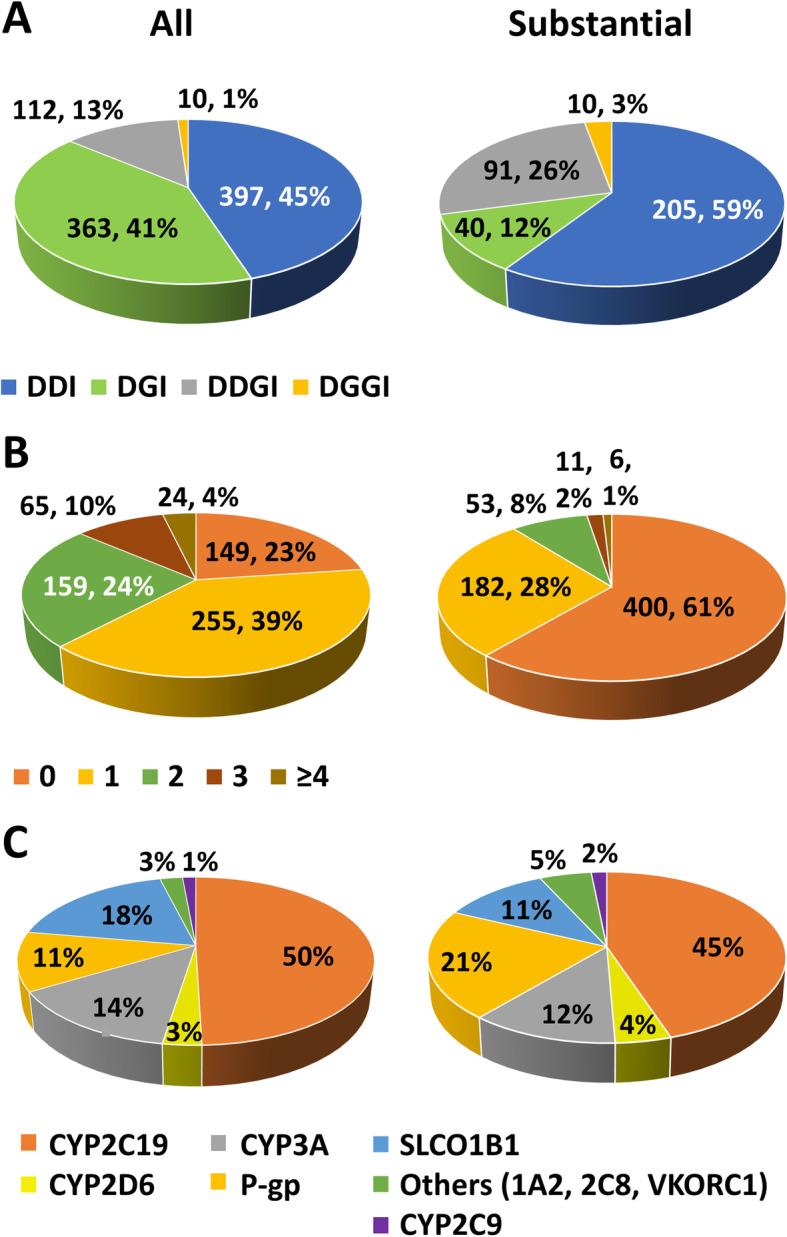
In the whole cohort, 727 (49.9%) patients had multimorbidity. Non-linear relationships between age and increasing comorbidities and decreasing coronary intervention were observed. There were 98.1% and 39.8% patients on ≥ 5 and ≥ 10 drugs, respectively (from n = 698); women received more non-cardiovascular drugs than men (median (IQR) 3 (1-5) vs 2 (1-4), p = 0.014). Overall, 98.7% patients had at least one actionable genotype. Within the interaction cohort, 882 interactions were identified in 503 patients (77.1%), of which 346 in 252 patients (38.7%) were substantial: 59.2%, 11.6%, 26.3%, and 2.9% substantial interactions were DDIs, DGIs, DDGIs, and DGGIs, respectively. CYP2C19 (49.5% of all interactions) and SLCO1B1 (18.4%) were involved in the largest number of interactions. Multimorbidity (p = 0.019) and number of drugs (p = 9.8 × 10) were both associated with patients having ≥ 1 substantial interaction. Multimorbidity (HR 1.76, 95% CI 1.10-2.82, p = 0.019), number of drugs (HR 1.10, 95% CI 1.04-1.16, p = 1.2 × 10), and age (HR 1.05, 95% CI 1.03-1.07, p = 8.9 × 10), but not drug interactions, were associated with increased subsequent major adverse cardiovascular events.
Multimorbidity, polypharmacy, and drug interactions are common after a NSTE-ACS. Replication of results is required; however, the high prevalence of DDGIs suggests integrating co-medications with genetic data will improve medicines optimisation.
患有共病的患者人数正在增加。本研究旨在评估非 ST 段抬高型急性冠状动脉综合征(NSTE-ACS)患者的多发病、药物使用以及药物和基因相互作用的程度。
在 1456 名因 NSTE-ACS 出院的患者中,评估了合并症和多发病(≥2 种慢性疾病)。其中,698 人出院时记录了完整的药物使用情况,652 人(“相互作用”队列)有药物使用和可操作的基因型,用于 CYP2B6、CYP2C9、CYP2C19、CYP2D6、CYP3A5、DPYD、F5、SLCO1B1、TPMT、UGT1A1 和 VKORC1。研究了以下药物相互作用:涉及 CYP(上述 CYP 加上 CYP1A2、CYP2C8 和 CYP3A4)、SLCO1B1 和 P-糖蛋白的药物-药物相互作用(DDIs);药物-基因相互作用(DGIs);药物-药物-基因相互作用(DDGIs);以及药物-基因-基因相互作用(DGGIs)。被预测为“显著”的相互作用定义如下:由于强抑制剂/诱导剂导致的 DDI、由于纯合子/复合杂合基因型导致的 DGIs,以及构成 DDI/DGI 的相互作用都以相同的方向影响受影响药物的 DDGIs/DGGIs。
在整个队列中,727 名(49.9%)患者患有多发病。观察到年龄与合并症增多和冠状动脉介入减少之间呈非线性关系。在 698 名患者中,分别有 98.1%和 39.8%的患者服用了≥5 和≥10 种药物(n=698);女性接受的非心血管药物多于男性(中位数(IQR)3(1-5)比 2(1-4),p=0.014)。总的来说,98.7%的患者至少有一种可操作的基因型。在相互作用队列中,在 503 名患者(77.1%)中发现了 882 种相互作用,其中 346 种相互作用(252 名患者中的 38.7%)是显著的:59.2%、11.6%、26.3%和 2.9%的显著相互作用分别为 DDI、DGIs、DDGIs 和 DGGIs。CYP2C19(所有相互作用的 49.5%)和 SLCO1B1(18.4%)涉及最多的相互作用。多发病(p=0.019)和药物数量(p=9.8×10)与患者有≥1 种显著相互作用相关。多发病(HR 1.76,95%CI 1.10-2.82,p=0.019)、药物数量(HR 1.10,95%CI 1.04-1.16,p=1.2×10)和年龄(HR 1.05,95%CI 1.03-1.07,p=8.9×10),而不是药物相互作用,与随后发生的主要不良心血管事件增加相关。
非 ST 段抬高型急性冠状动脉综合征后多发病、多药治疗和药物相互作用很常见。需要复制结果;然而,DDGIs 的高患病率表明,将共用药与遗传数据相结合将改善药物优化。