Foundation for Innovative New Diagnostics (FIND) Campus Biotech, Chemin des Mines 9, 1202, Geneva, Switzerland.
Big Data Institute, University of Oxford, Old Road Campus, Oxford, OX3 7LF, UK.
Trials. 2020 Nov 25;21(1):974. doi: 10.1186/s13063-020-04897-9.
The management of acute febrile illnesses places a heavy burden on clinical services in many low- and middle-income countries (LMICs). Bacterial and viral aetiologies of acute fevers are often clinically indistinguishable and, in the absence of diagnostic tests, the 'just-in-case' use of antibiotics by many health workers has become common practice, which has an impact on drug-resistant infections. Our study aims to answer the following question: in patients with undifferentiated febrile illness presenting to outpatient clinics/peripheral health centres in LMICs, can we demonstrate an improvement in clinical outcomes and reduce unnecessary antibiotic prescription over current practice by using a combination of simple, accurate diagnostic tests, clinical algorithms, and training and communication (intervention package)?
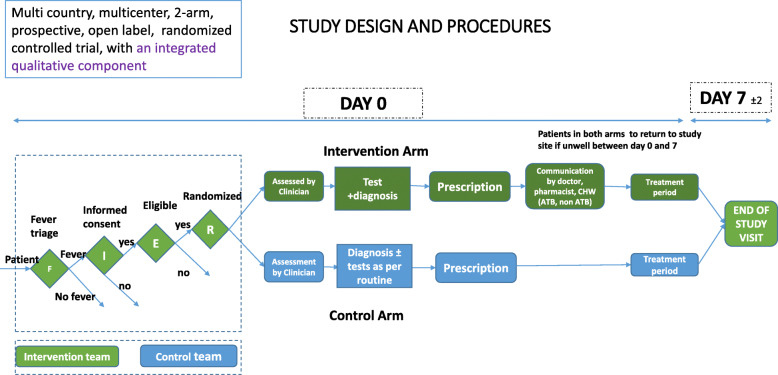
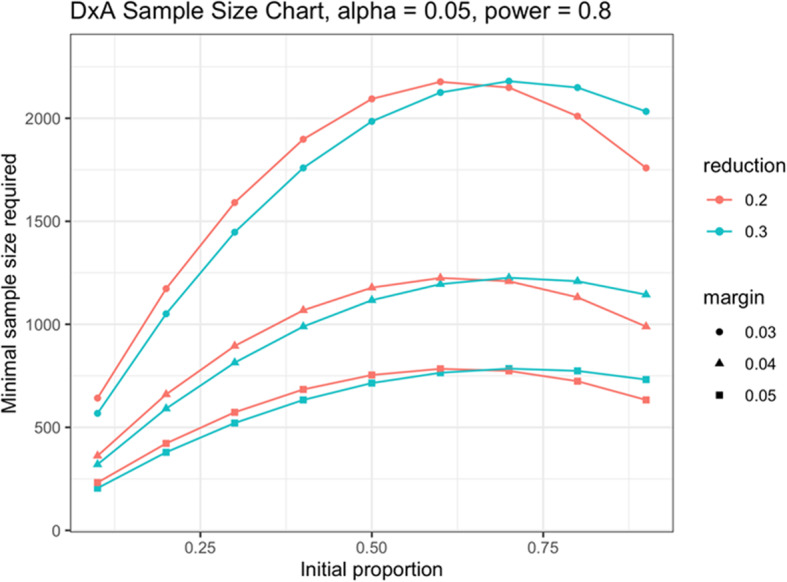
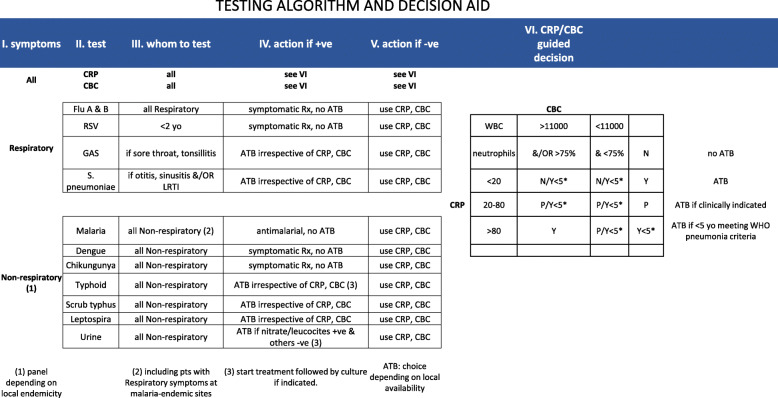
We designed a randomized, controlled clinical trial to evaluate the impact of our intervention package on clinical outcomes and antibiotic prescription rates in acute febrile illnesses. Available, point-of-care, pathogen-specific and non-pathogen specific (host markers), rapid diagnostic tests (RDTs) included in the intervention package were selected based on pre-defined criteria. Nine clinical study sites in six countries (Burkina Faso, Ghana, India, Myanmar, Nepal and Uganda), which represent heterogeneous outpatient care settings, were selected. We considered the expected seasonal variations in the incidence of acute febrile illnesses across all the sites by ensuring a recruitment period of 12 months. A master protocol was developed and adapted for country-specific ethical submissions. Diagnostic algorithms and choice of RDTs acknowledged current data on aetiologies of acute febrile illnesses in each country. We included a qualitative evaluation of drivers and/or deterrents of uptake of new diagnostics and antibiotic use for acute febrile illnesses. Sample size estimations were based on historical site data of antibiotic prescription practices for malarial and non-malarial acute fevers. Overall, 9 semi-independent studies will enrol a minimum of 21,876 patients and an aggregate data meta-analysis will be conducted on completion.
This study is expected to generate vital evidence needed to inform policy decisions on the role of rapid diagnostic tests in the clinical management of acute febrile illnesses, with a view to controlling the rise of antimicrobial resistance in LMICs.
Clinicaltrials.gov NCT04081051 . Registered on 6 September 2019. Protocol version 1.4 dated 20 December 2019.
急性发热性疾病的管理给许多低收入和中等收入国家(LMICs)的临床服务带来了沉重负担。急性发热的细菌和病毒病因在临床上通常难以区分,而且在缺乏诊断测试的情况下,许多卫生工作者出于“以防万一”的考虑常规使用抗生素,这对耐药感染产生了影响。我们的研究旨在回答以下问题:在 LMICs 的门诊/基层医疗中心就诊的未明确诊断的发热患者中,通过使用简单、准确的诊断测试、临床算法以及培训和沟通(干预包),我们能否在临床结局方面取得改善并减少不必要的抗生素处方?
我们设计了一项随机对照临床试验,以评估干预包对急性发热性疾病的临床结局和抗生素处方率的影响。干预包中包含的可用、即时、病原体特异性和非病原体特异性(宿主标志物)、快速诊断测试(RDTs)是根据预先定义的标准选择的。在六个国家(布基纳法索、加纳、印度、缅甸、尼泊尔和乌干达)的九个临床研究地点中进行了选择,这些地点代表了不同的门诊护理环境。我们通过确保 12 个月的招募期来考虑所有地点急性发热性疾病发病率的预期季节性变化。制定了一份总体方案,并根据各国的具体伦理要求进行了调整。诊断算法和 RDT 的选择承认了每个国家急性发热性疾病病因的当前数据。我们还对新诊断和急性发热性疾病抗生素使用的采用的驱动因素和/或阻碍因素进行了定性评估。样本量估算基于历史站点的抗生素处方实践数据,用于疟疾和非疟疾性急性发热。总体而言,9 项半独立研究将招募至少 21876 名患者,完成后将进行汇总数据荟萃分析。
这项研究预计将产生急需的证据,为快速诊断测试在急性发热性疾病临床管理中的作用提供决策依据,以期控制 LMICs 中抗菌药物耐药性的上升。
Clinicaltrials.gov NCT04081051。于 2019 年 9 月 6 日注册。2019 年 12 月 20 日修订第 1.4 版方案。