Clinical Research Unit of Nanoro, Institut de Recherche en Sciences de la Santé, 11 BP 218, Ouaga CMS 11 , Nanoro, Burkina Faso.
FIND, Geneva, Switzerland.
BMC Infect Dis. 2024 Aug 27;24(1):870. doi: 10.1186/s12879-024-09787-y.
To assess the impact of an intervention package on the prescription of antibiotic and subsequently the rate of clinical recovery for non-severe acute febrile illnesses at primary health centers.
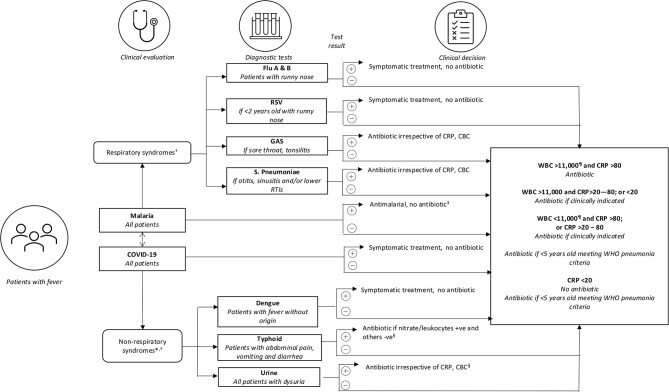
Patients over 6 months of age presenting to primary health care centres with fever or history of fever within the past 7 days were randomized to receive either the intervention package constituted of point-of-care tests including COVID-19 antigen tests, a diagnostic algorithm and training and communication packages, or the standard practice. The primary outcomes were antibiotic prescriptions at Day 0 (D0) and the clinical recovery at Day 7 (D7). Secondary outcomes were non-adherence of participants and parents/caregivers to prescriptions, health workers' non-adherence to the algorithm, and the safety of the intervention.
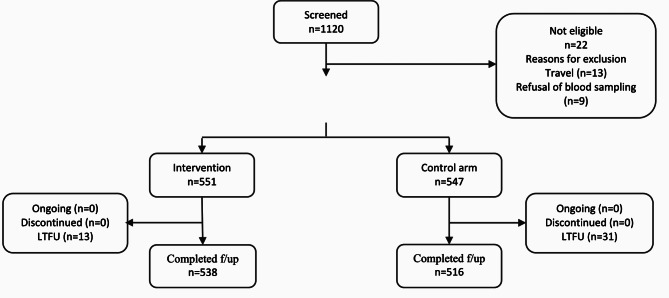
A total of 1098 patients were enrolled. 551 (50.2%) were randomized to receive the intervention versus 547 (49.8%) received standard care. 1054 (96.0%) completed follow-up and all of them recovered at D7 in both arms. The proportion of patients with antibiotic prescriptions at D0 were 33.2% (183/551) in the intervention arm versus 58.1% (318/547) under standard care, risk difference (RD) -24.9 (95% CI -30.6 to -19.2, p < 0.001), corresponding to one more antibiotic saved every four (95% CI: 3 to 5) consultations. This reduction was also statistically significant in children from 6 to 59 months (RD -34.5; 95% CI -41.7 to -27.3; p < 0.001), patients over 18 years (RD -35.9; 95%CI -58.5 to -13.4; p = 0.002), patients with negative malaria test (RD -46.9; 95% CI -53.9 to -39.8; p < 0.001), those with a respiratory diagnosis (RD -48.9; 95% CI -56.9 to -41.0, p < 0.001) and those not vaccinated against COVID-19 (-24.8% 95%CI -30.7 to -18.9, p-value: <0.001). A significant reduction in non-adherence to prescription by patients was reported (RD -7.1; 95% CI -10.9 to -3.3; p < 0.001).
The intervention was associated with significant reductions of antibiotic prescriptions and non-adherence, chiefly among patients with non-malaria fever, those with respiratory symptoms and children below 5 years of age. The addition of COVID-19 testing did not have a major impact on antibiotic use at primary health centers.
Clinitrial.gov; NCT04081051 registered on 06/09/2019.
评估干预方案对初级保健中心非严重急性发热疾病抗生素处方的影响,以及临床康复率。
6 个月以上的发热患者或过去 7 天内有发热史的患者在初级保健中心就诊,随机接受包括 COVID-19 抗原检测在内的即时检测、诊断算法和培训与沟通方案的干预包,或标准治疗。主要结局是第 0 天(D0)的抗生素处方和第 7 天(D7)的临床康复情况。次要结局是参与者和家长/看护人对处方的不依从性、卫生工作者对算法的不依从性以及干预的安全性。
共纳入 1098 例患者,551 例(50.2%)接受干预治疗,547 例(49.8%)接受标准护理。1054 例(96.0%)完成随访,所有患者在第 7 天均痊愈。干预组第 0 天(D0)有抗生素处方的患者比例为 33.2%(183/551),标准护理组为 58.1%(318/547),差异为-24.9%(95%CI-30.6 至-19.2,p<0.001),即每 4 次(95%CI:3 至 5)就诊可节省 1 种抗生素。这一减少在 6 至 59 个月的儿童(RD-34.5;95%CI-41.7 至-27.3;p<0.001)、18 岁以上患者(RD-35.9;95%CI-58.5 至-13.4;p=0.002)、疟疾检测阴性患者(RD-46.9;95%CI-53.9 至-39.8;p<0.001)、有呼吸道诊断患者(RD-48.9;95%CI-56.9 至-41.0,p<0.001)和未接种 COVID-19 疫苗患者(RD-24.8%;95%CI-30.7 至-18.9,p 值<0.001)中均有统计学意义。报告称,患者对处方的不依从性显著降低(RD-7.1;95%CI-10.9 至-3.3;p<0.001)。
该干预方案与抗生素处方和不依从性的显著减少有关,主要发生在非疟疾发热患者、有呼吸道症状的患者和 5 岁以下儿童中。在初级保健中心添加 COVID-19 检测并没有对抗生素的使用产生重大影响。
Clinitrial.gov;NCT04081051 于 2019 年 9 月 6 日注册。