Department of Medical Oncology, Dana-Farber Cancer Institute, Boston, Massachusetts.
Department of Pathology, Brigham and Women's Hospital, Boston, Massachusetts.
Clin Cancer Res. 2021 Jan 1;27(1):276-287. doi: 10.1158/1078-0432.CCR-20-2291. Epub 2020 Nov 25.
Dexamethasone, a uniquely potent corticosteroid, is frequently administered to patients with brain tumors to decrease tumor-associated edema, but limited data exist describing how dexamethasone affects the immune system systemically and intratumorally in patients with glioblastoma (GBM), particularly in the context of immunotherapy.
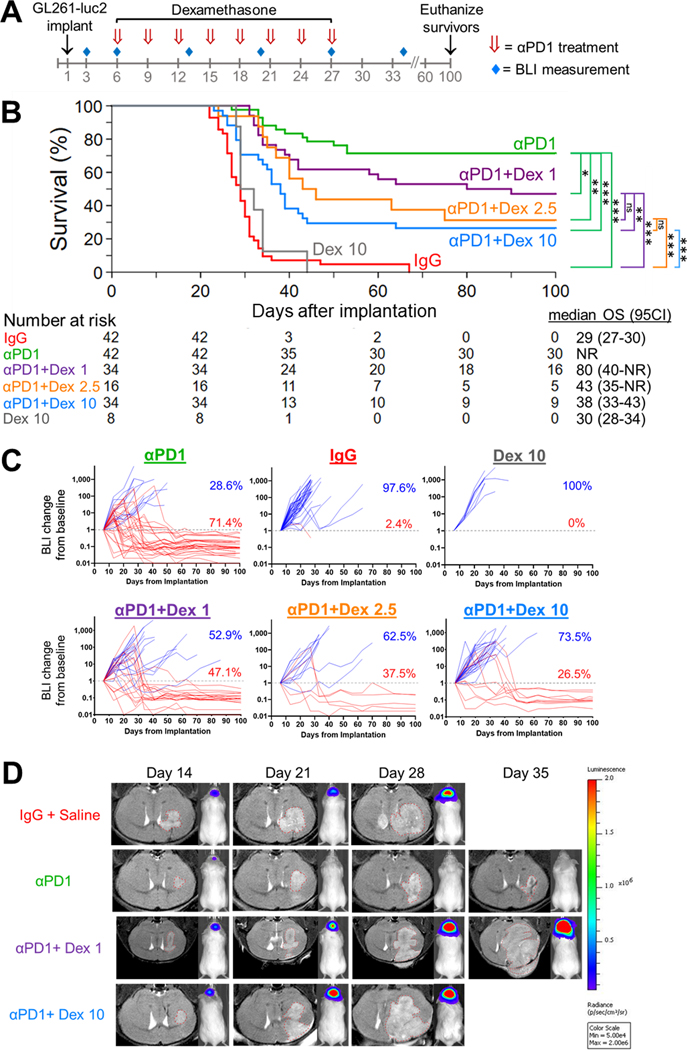
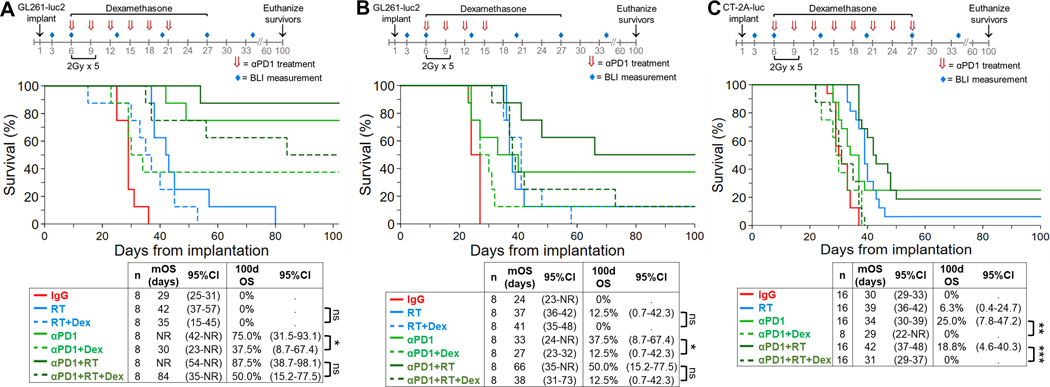
We evaluated the dose-dependent effects of dexamethasone when administered with programmed cell death 1 (PD-1) blockade and/or radiotherapy in immunocompetent C57BL/6 mice with syngeneic GL261 and CT-2A GBM tumors. Clinically, the effect of dexamethasone on survival was evaluated in 181 patients with isocitrate dehydrogenase (IDH) wild-type GBM treated with PD-(L)1 blockade, with adjustment for relevant prognostic factors.
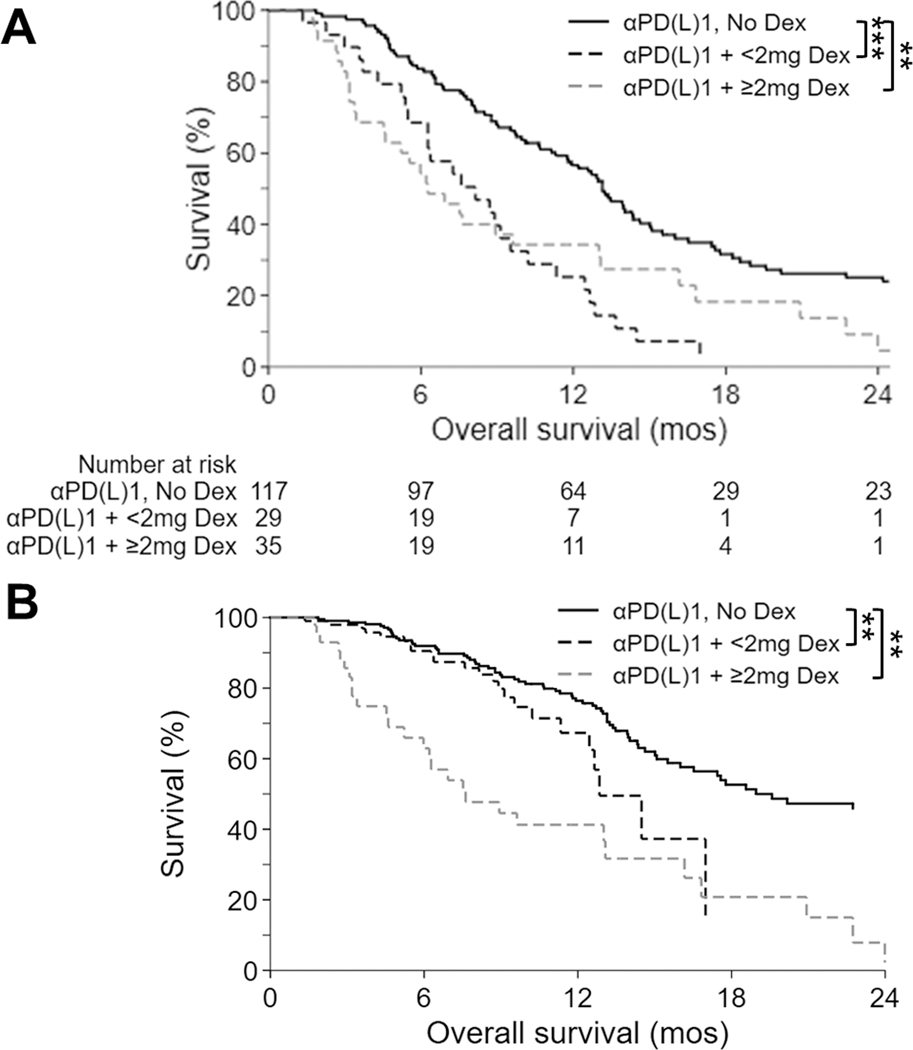
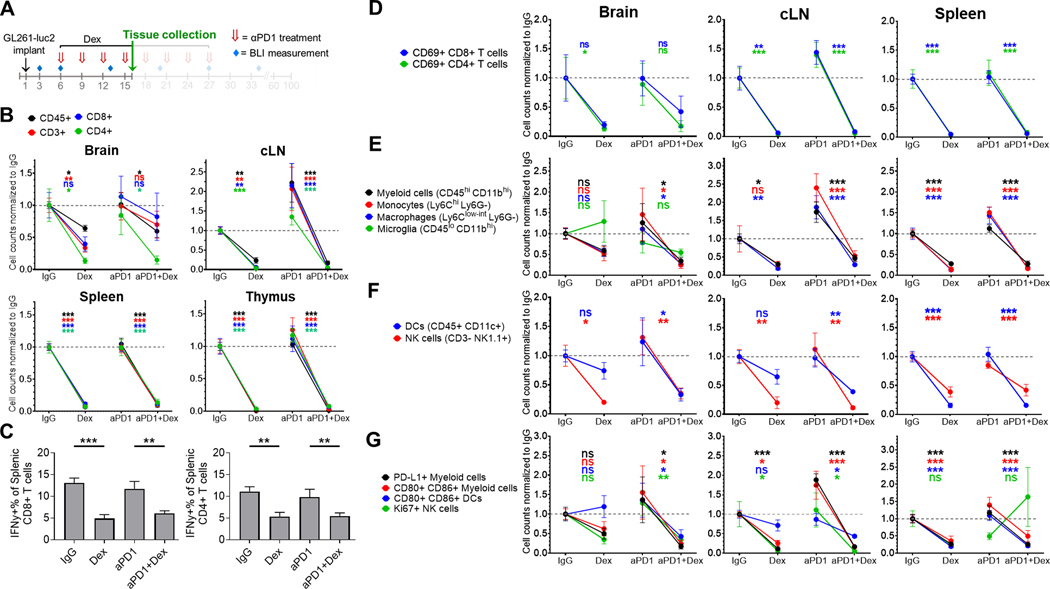
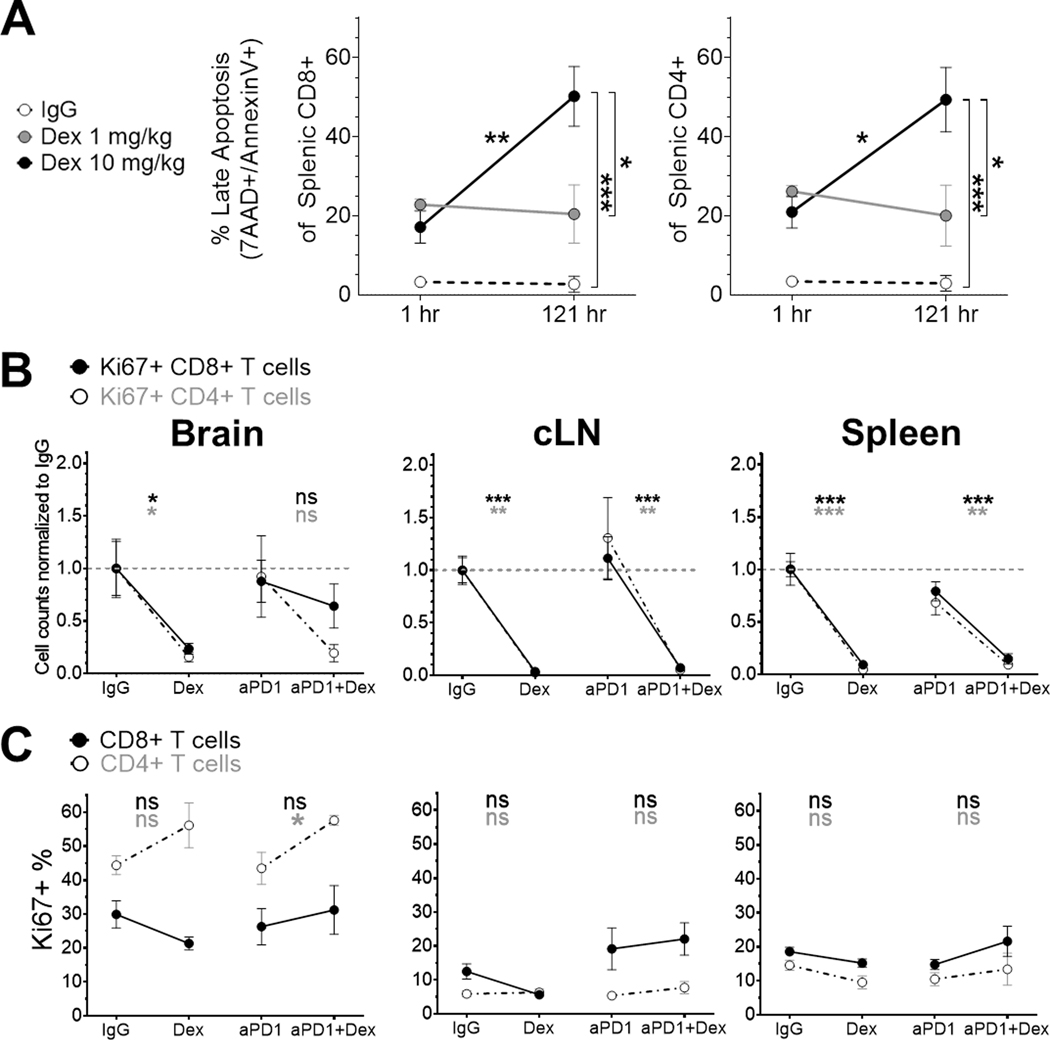
Despite the inherent responsiveness of GL261 to immune checkpoint blockade, concurrent dexamethasone administration with anti-PD-1 therapy reduced survival in a dose-dependent manner. Concurrent dexamethasone also abrogated survival following anti-PD-1 therapy with or without radiotherapy in immune-resistant CT-2A models. Dexamethasone decreased T-lymphocyte numbers by increasing apoptosis, in addition to decreasing lymphocyte functional capacity. Myeloid and natural killer cell populations were also generally reduced by dexamethasone. Thus, dexamethasone appears to negatively affect both adaptive and innate immune responses. As a clinical correlate, a retrospective analysis of 181 consecutive patients with IDH wild-type GBM treated with PD-(L)1 blockade revealed poorer survival among those on baseline dexamethasone. Upon multivariable adjustment with relevant prognostic factors, baseline dexamethasone administration was the strongest predictor of poor survival [reference, no dexamethasone; <2 mg HR, 2.16; 95% confidence interval (CI), 1.30-3.68; = 0.003 and ≥2 mg HR, 1.97; 95% CI, 1.23-3.16; = 0.005].
Our preclinical and clinical data indicate that concurrent dexamethasone therapy may be detrimental to immunotherapeutic approaches for patients with GBM.
地塞米松是一种具有独特效力的皮质类固醇,常用于降低脑肿瘤患者的肿瘤相关水肿,但关于地塞米松如何影响胶质母细胞瘤(GBM)患者全身和肿瘤内的免疫系统的数据有限,特别是在免疫治疗的背景下。
我们评估了地塞米松在免疫活性 C57BL/6 小鼠中与程序性细胞死亡 1(PD-1)阻断和/或放疗联合使用时的剂量依赖性效应,这些小鼠患有同源 GL261 和 CT-2A GBM 肿瘤。临床上,通过调整相关预后因素,评估了地塞米松对 181 例异柠檬酸脱氢酶(IDH)野生型 GBM 患者接受 PD-(L)1 阻断治疗的生存影响。
尽管 GL261 对免疫检查点阻断具有固有反应性,但地塞米松与抗 PD-1 治疗联合使用会以剂量依赖性方式降低生存。在免疫抵抗的 CT-2A 模型中,地塞米松联合抗 PD-1 治疗和/或放疗也会缩短生存。地塞米松通过增加细胞凋亡来减少 T 淋巴细胞数量,此外还降低了淋巴细胞功能能力。地塞米松还普遍减少了髓样细胞和自然杀伤细胞群体。因此,地塞米松似乎会对适应性和固有免疫反应产生负面影响。作为临床相关性,对接受 PD-(L)1 阻断治疗的 181 例连续 IDH 野生型 GBM 患者进行回顾性分析显示,基线时使用地塞米松的患者生存较差。在校正相关预后因素后,基线时使用地塞米松是不良生存的最强预测因素[参考,无地塞米松;<2 mg HR,2.16;95%置信区间(CI),1.30-3.68; = 0.003 和≥2 mg HR,1.97;95% CI,1.23-3.16; = 0.005]。
我们的临床前和临床数据表明,同时使用地塞米松治疗可能对 GBM 患者的免疫治疗方法不利。