Department of Medical Sciences, Endocrine Oncology, Uppsala University, Uppsala, Sweden.
Department of Oncology, Ryhov County Hospital, Jönköping, Sweden.
Endocrine. 2021 Jun;72(3):893-904. doi: 10.1007/s12020-020-02534-8. Epub 2020 Nov 26.
Small intestinal neuroendocrine tumours (siNETs) with a Ki-67 proliferation index between 3 and 20% belong to WHO grade 2. Response to treatment may be monitored by blood chromogranin A (CgA) and urine 5-hydroxyindoleacetic acid (5HIAA). The aim of this retrospective study was to investigate the prognostic value of baseline CgA and 5HIAA and of the early biochemical response to treatment, and to compare different cut-off values used in the literature.
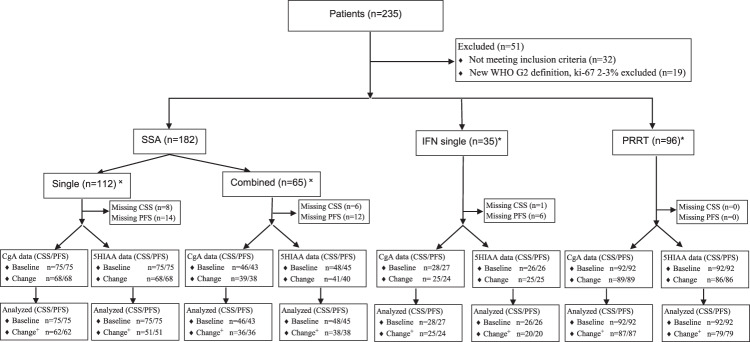
A retrospective cohort study of 184 patients with siNET Grade 2 treated with somatostatin analogues (SSA), interferon-alpha (IFN) or peptide receptor radionuclide therapy (PRRT).
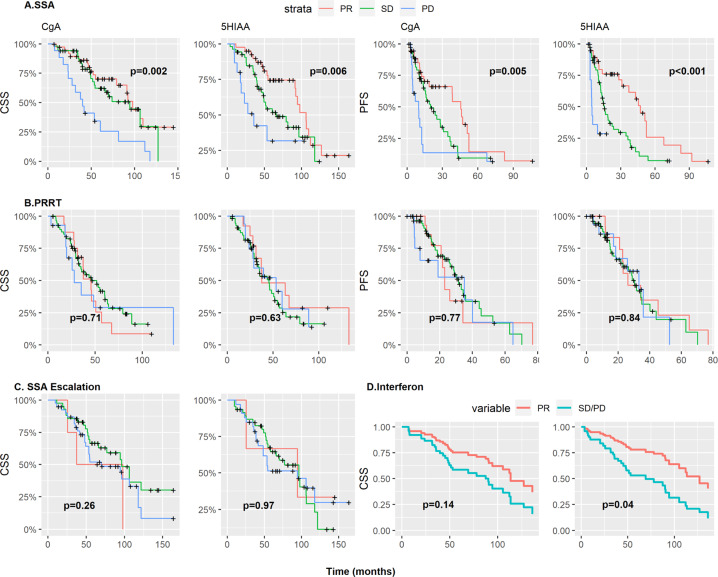
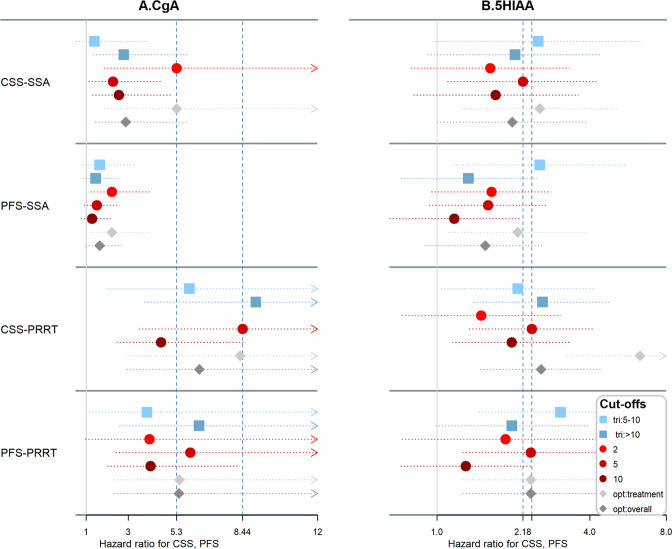
Baseline CgA was a statistically significant prognostic marker for both cancer-specific survival (CSS) and progression-free survival (PFS). A cut-off of 5 × ULN (upper limit of normal) was best discriminative in most cases, but 2 × ULN discriminated better for SSA. Baseline 5HIAA was a prognostic marker for CSS in treatment with IFN and PRRT, but not for single SSA. Early changes of CgA and 5HIAA correlated well with CSS (HR 3.18, 95% CI 1.82-5.56 and HR 1.47, 95% CI 1.16-1.86) and PFS (HR 3.08, 95% CI 1.86-5.10 and HR 1.37, 95% CI 1.11-1.68) for SSA, but not for PRRT.
Baseline CgA and to a lesser extent 5HIAA are associated with CSS irrespective of treatment used, and with PFS after PRRT, and 5 × ULN provides best discrimination in many, but not all, cases. Early reductions of CgA and 5HIAA are prognostic for treatment with SSA, but not PRRT.
Ki-67 增殖指数在 3%至 20%之间的小肠神经内分泌肿瘤(siNETs)属于世界卫生组织(WHO)分级 2 级。可以通过血液嗜铬粒蛋白 A(CgA)和尿液 5-羟吲哚乙酸(5HIAA)来监测治疗反应。本回顾性研究旨在探讨基线 CgA 和 5HIAA 的预后价值以及对治疗的早期生化反应,并比较文献中使用的不同截止值。
对 184 例接受生长抑素类似物(SSA)、干扰素-α(IFN)或肽受体放射性核素治疗(PRRT)治疗的 siNET 2 级患者进行回顾性队列研究。
基线 CgA 是癌症特异性生存(CSS)和无进展生存(PFS)的统计学显著预后标志物。在大多数情况下,5×ULN(正常值上限)的截止值具有最佳的区分能力,但对于 SSA,2×ULN 的区分能力更好。基线 5HIAA 是 IFN 和 PRRT 治疗 CSS 的预后标志物,但不是 SSA 单一治疗的预后标志物。CgA 和 5HIAA 的早期变化与 CSS(HR 3.18,95%CI 1.82-5.56 和 HR 1.47,95%CI 1.16-1.86)和 PFS(HR 3.08,95%CI 1.86-5.10 和 HR 1.37,95%CI 1.11-1.68)具有良好的相关性,而与 SSA 治疗的相关性不佳。
基线 CgA ,在一定程度上还有 5HIAA,与 CSS 相关,与 PRRT 后的 PFS 相关,5×ULN 在许多情况下(但并非所有情况下)提供最佳区分度。CgA 和 5HIAA 的早期降低与 SSA 的治疗相关,但与 PRRT 无关。