Department of Medical Oncology, Fondazione IRCCS Istituto Nazionale dei Tumori di Milano, European Neuroendocrine Tumor Society (ENETS) Center of Excellence, Milan, Italy.
Oncologia Clinica e Sperimentale Sarcomi e Tumori Rari, Istituto Nazionale Tumori IRCCS, Fondazione G. Pascale, Naples, Italy.
JAMA Netw Open. 2022 Feb 1;5(2):e220290. doi: 10.1001/jamanetworkopen.2022.0290.
Data about the optimal timing for the initiation of peptide receptor radionuclide therapy (PRRT) for advanced, well-differentiated enteropancreatic neuroendocrine tumors are lacking.
To evaluate the association of upfront PRRT vs upfront chemotherapy or targeted therapy with progression-free survival (PFS) among patients with advanced enteropancreatic neuroendocrine tumors who experienced disease progression after treatment with somatostatin analogues (SSAs).
DESIGN, SETTING, AND PARTICIPANTS: This retrospective, multicenter cohort study analyzed the clinical records from 25 Italian oncology centers for patients aged 18 years or older who had unresectable, locally advanced or metastatic, well-differentiated, grades 1 to 3 enteropancreatic neuroendocrine tumors and received either PRRT or chemotherapy or targeted therapy after experiencing disease progression after treatment with SSAs between January 24, 2000, and July 1, 2020. Propensity score matching was done to minimize the selection bias.
Upfront PRRT or upfront chemotherapy or targeted therapy.
The main outcome was the difference in PFS among patients who received upfront PRRT vs among those who received upfront chemotherapy or targeted therapy. A secondary outcome was the difference in overall survival between these groups. Hazard ratios (HRs) were fitted in a multivariable Cox proportional hazards regression model to adjust for relevant factors associated with PFS and were corrected for interaction with these factors.
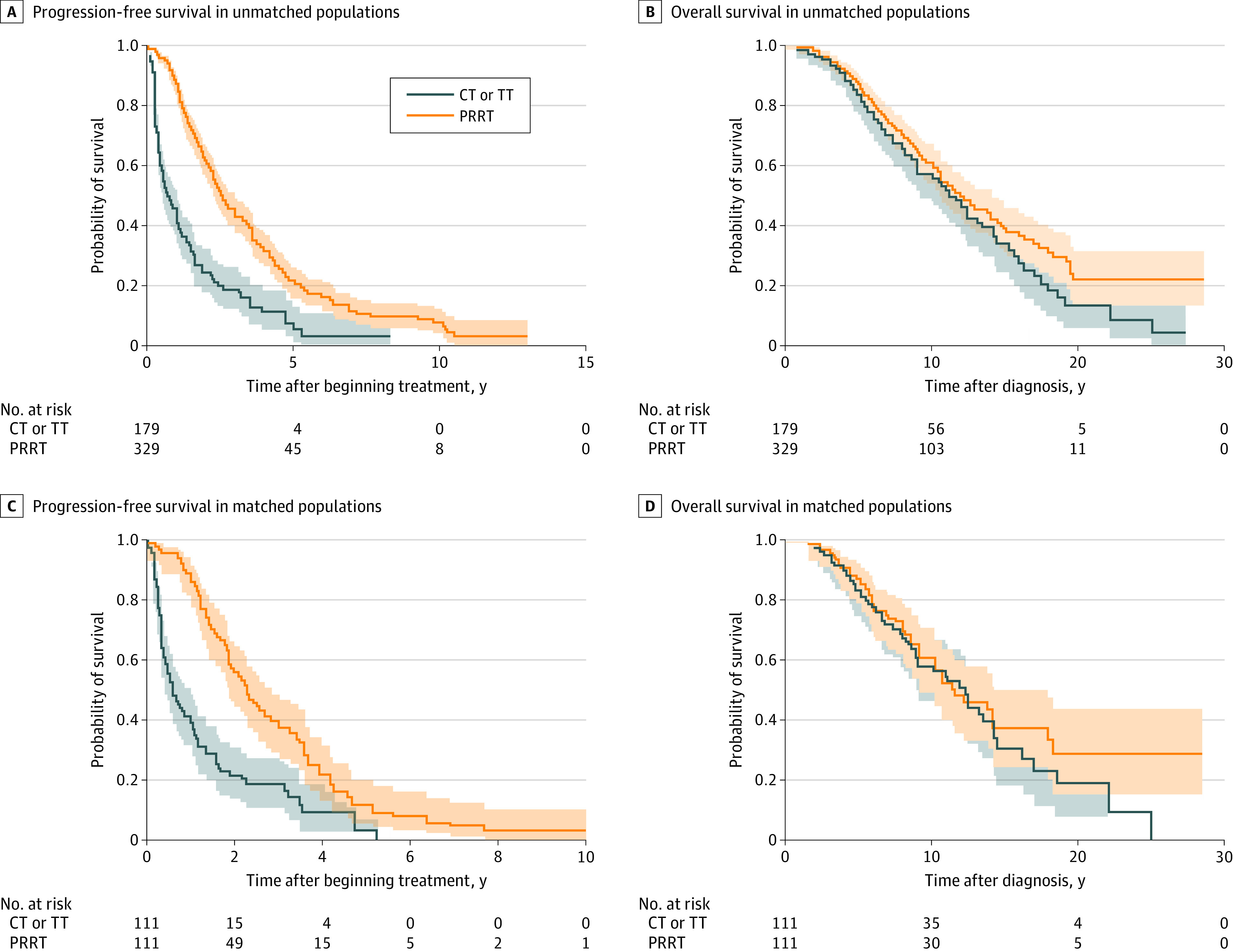
Of 508 evaluated patients (mean ([SD] age, 55.7 [0.5] years; 278 [54.7%] were male), 329 (64.8%) received upfront PRRT and 179 (35.2%) received upfront chemotherapy or targeted therapy. The matched group included 222 patients (124 [55.9%] male; mean [SD] age, 56.1 [0.8] years), with 111 in each treatment group. Median PFS was longer in the PRRT group than in the chemotherapy or targeted therapy group in the unmatched (2.5 years [95% CI, 2.3-3.0 years] vs 0.7 years [95% CI, 0.5-1.0 years]; HR, 0.35 [95% CI, 0.28-0.44; P < .001]) and matched (2.2 years [95% CI, 1.8-2.8 years] vs 0.6 years [95% CI, 0.4-1.0 years]; HR, 0.37 [95% CI, 0.27-0.51; P < .001]) populations. No significant differences were shown in median overall survival between the PRRT and chemotherapy or targeted therapy groups in the unmatched (12.0 years [95% CI, 10.7-14.1 years] vs 11.6 years [95% CI, 9.1-13.4 years]; HR, 0.81 [95% CI, 0.62-1.06; P = .11]) and matched (12.2 years [95% CI, 9.1-14.2 years] vs 11.5 years [95% CI, 9.2-17.9 years]; HR, 0.83 [95% CI, 0.56-1.24; P = .36]) populations. The use of upfront PRRT was independently associated with improved PFS (HR, 0.37; 95% CI, 0.26-0.51; P < .001) in multivariable analysis. After adjustment of values for interaction, upfront PRRT was associated with longer PFS regardless of tumor functional status (functioning: adjusted HR [aHR], 0.39 [95% CI, 0.27-0.57]; nonfunctioning: aHR, 0.29 [95% CI, 0.16-0.56]), grade of 1 to 2 (grade 1: aHR, 0.21 [95% CI, 0.12-0.34]; grade 2: aHR, 0.52 [95% CI, 0.29-0.73]), and site of tumor origin (pancreatic: aHR, 0.41 [95% CI, 0.24-0.61]; intestinal: aHR, 0.19 [95% CI, 0.11-0.43]) (P < .001 for all). Conversely, the advantage was not retained in grade 3 tumors (aHR, 0.31; 95% CI, 0.12-1.37; P = .13) or in tumors with a Ki-67 proliferation index greater than 10% (aHR, 0.73; 95% CI, 0.29-1.43; P = .31).
In this cohort study, treatment with upfront PRRT in patients with enteropancreatic neuroendocrine tumors who had experienced disease progression with SSA treatment was associated with significantly improved survival outcomes compared with upfront chemotherapy or targeted therapy. Further research is needed to investigate the correct strategy, timing, and optimal specific sequence of these therapeutic options.
重要性:缺乏关于肽受体放射性核素疗法 (PRRT) 在晚期、分化良好的肠胰神经内分泌肿瘤患者中的最佳起始时间的数据,这些患者在接受生长抑素类似物 (SSA) 治疗后疾病进展。
目的:评估在接受 SSA 治疗后疾病进展的晚期肠胰神经内分泌肿瘤患者中,与 upfront 化疗或靶向治疗相比, upfront PRRT 与无进展生存期 (PFS) 的相关性。
设计、地点和参与者:这项回顾性、多中心队列研究分析了来自 25 家意大利肿瘤中心的临床记录,这些患者年龄在 18 岁及以上,患有不可切除的局部晚期或转移性、分化良好、1 至 3 级的肠胰神经内分泌肿瘤,在接受 SSA 治疗后疾病进展,随后接受 PRRT 或化疗或靶向治疗。采用倾向性评分匹配来尽量减少选择偏倚。
暴露: upfront PRRT 或 upfront 化疗或靶向治疗。
主要结果和测量:主要结局是接受 upfront PRRT 的患者与接受 upfront 化疗或靶向治疗的患者之间的 PFS 差异。次要结局是这些组之间总生存期的差异。多变量 Cox 比例风险回归模型拟合了风险比 (HR),以调整与 PFS 相关的相关因素,并对与这些因素的交互作用进行了校正。
结果:在 508 例评估患者中(平均[SD]年龄 55.7[0.5]岁;278[54.7%]为男性),329 例(64.8%)接受 upfront PRRT,179 例(35.2%)接受 upfront 化疗或靶向治疗。匹配组包括 222 例患者(124[55.9%]为男性;平均[SD]年龄 56.1[0.8]岁),每组各有 111 例。未匹配组中 PRRT 组的中位 PFS 长于化疗或靶向治疗组(2.5 年[95%CI,2.3-3.0 年] vs 0.7 年[95%CI,0.5-1.0 年];HR,0.35[95%CI,0.28-0.44;P<0.001])和匹配组(2.2 年[95%CI,1.8-2.8 年] vs 0.6 年[95%CI,0.4-1.0 年];HR,0.37[95%CI,0.27-0.51;P<0.001])。在未匹配组(12.0 年[95%CI,10.7-14.1 年] vs 11.6 年[95%CI,9.1-13.4 年];HR,0.81[95%CI,0.62-1.06;P=0.11])和匹配组(12.2 年[95%CI,9.1-14.2 年] vs 11.5 年[95%CI,9.2-17.9 年];HR,0.83[95%CI,0.56-1.24;P=0.36])中,PRRT 组与化疗或靶向治疗组之间的中位总生存期无显著差异。多变量分析显示, upfront PRRT 与改善的 PFS 独立相关(HR,0.37;95%CI,0.26-0.51;P<0.001)。调整交互作用的值后,无论肿瘤功能状态如何(功能性:调整后的 HR[aHR],0.39[95%CI,0.27-0.57];非功能性:aHR,0.29[95%CI,0.16-0.56])、分级为 1 至 2 级(分级 1:aHR,0.21[95%CI,0.12-0.34];分级 2:aHR,0.52[95%CI,0.29-0.73])和肿瘤起源部位(胰腺:aHR,0.41[95%CI,0.24-0.61];肠:aHR,0.19[95%CI,0.11-0.43])(所有 P<0.001), upfront PRRT 都与更长的 PFS 相关。然而,在 3 级肿瘤(aHR,0.31;95%CI,0.12-1.37;P=0.13)或 Ki-67 增殖指数大于 10%的肿瘤(aHR,0.73;95%CI,0.29-1.43;P=0.31)中,这种优势并未保留。
结论和相关性:在这项队列研究中,与 upfront 化疗或靶向治疗相比,在接受 SSA 治疗后疾病进展的肠胰神经内分泌肿瘤患者中使用 upfront PRRT 治疗与显著改善的生存结果相关。需要进一步研究以调查这些治疗选择的正确策略、时机和最佳特定顺序。