Endo Shungo, Kumamoto K, Enomoto T, Koizumi K, Kato H, Saida Y
Department of Coloproctology, Aizu Medical Center, Fukushima Medical University, Aizu-Wakamatsu City, Fukushima, 969-3492, Japan.
Department of Surgery, Toho University Ohashi Medical Center, Tokyo, Japan.
Int J Colorectal Dis. 2021 May;36(5):987-998. doi: 10.1007/s00384-020-03806-5. Epub 2020 Nov 27.
Advances in endoscopic technology have led to the reevaluation of self-expandable metallic stent (SEMS) placement as a bridge-to-surgery (BTS) in patients with obstructive colorectal cancer. In Japan, after inclusion of SEMS placement as a BTS in the medical insurance coverage in 2012, this procedure has been increasingly performed. However, a transanal decompression tube (TADT) placement has been used as a BTS. We aimed to retrospectively evaluate the optimal strategy for obstructive left-sided colorectal cancer (OLCRC) by comparing SEMS and TADT placement with emergency surgery.
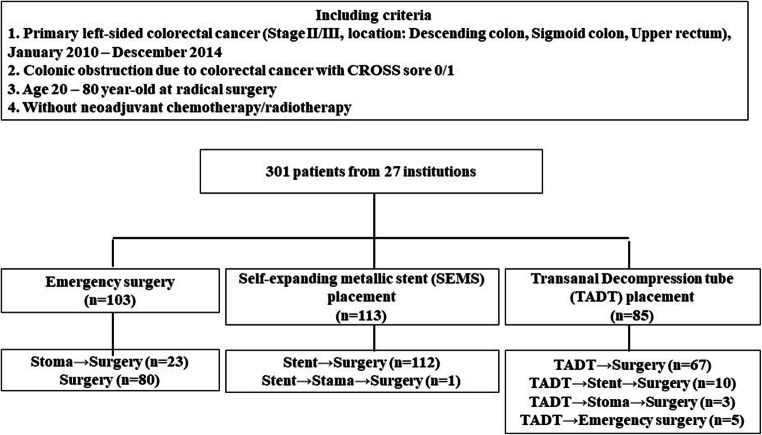
We included 301 patients with stage II and III OLCRC from 27 institutions. The study patients were divided into Surgery group (emergency surgery, n = 103), SEMS group (BTS by SEMS, n = 113), and TADT group (BTS by TADT, n = 85). We compared the survival and perioperative outcomes of patients in the Surgery group as a standard treatment with those in the SEMS and TADT groups.
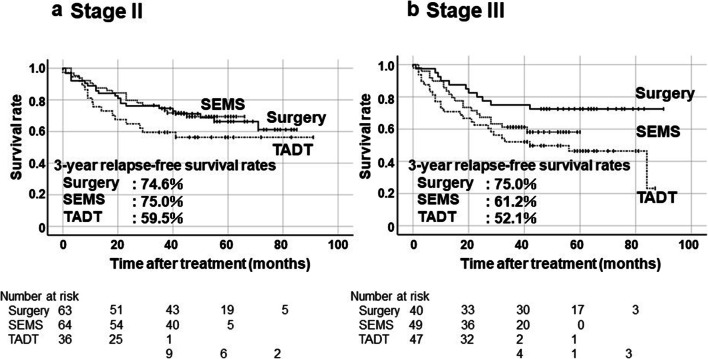
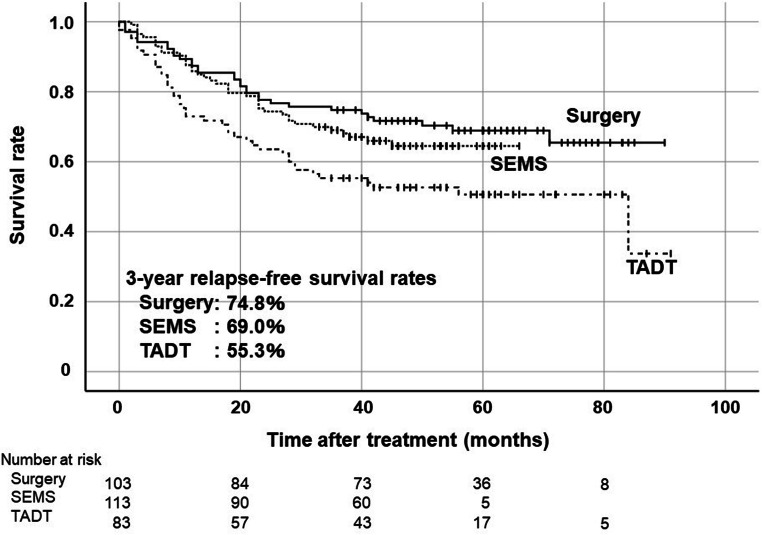
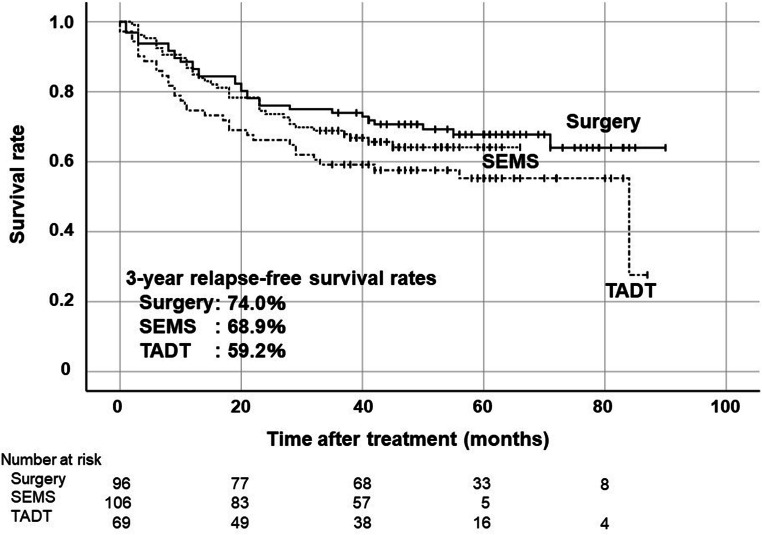
The 3-year relapse-free survival rate in patients in the Surgery group was 74.8%, while that in patients in the SEMS group and TADT group were 69.0% (p = 0.39) and 55.3% (p = 0.006), respectively. The technical success rate was not statistically different, but the clinical success rate was significantly higher in the SEMS group than in the TADT group (p = 0.0040). With regard to postoperative complications after curative surgery, the SEMS group had significantly lower of complications (≥ grade 2) than the Surgery group (p = 0.022).
Patients who underwent SEMS placement for OLCRC had similar oncological outcomes to patients who underwent emergency surgery.
内镜技术的进步促使人们重新评估自膨式金属支架(SEMS)置入术作为梗阻性结直肠癌患者手术过渡(BTS)的方法。在日本,自2012年SEMS置入术被纳入医疗保险覆盖范围作为手术过渡方法后,该手术的开展越来越多。然而,经肛门减压管(TADT)置入术也被用作手术过渡方法。我们旨在通过比较SEMS和TADT置入术与急诊手术,回顾性评估梗阻性左侧结直肠癌(OLCRC)的最佳治疗策略。
我们纳入了来自27家机构的301例II期和III期OLCRC患者。研究患者分为手术组(急诊手术,n = 103)、SEMS组(通过SEMS进行手术过渡,n = 113)和TADT组(通过TADT进行手术过渡,n = 85)。我们将手术组患者作为标准治疗与SEMS组和TADT组患者的生存及围手术期结局进行比较。
手术组患者的3年无复发生存率为74.8%,而SEMS组和TADT组患者的3年无复发生存率分别为69.0%(p = 0.39)和55.3%(p = 0.006)。技术成功率无统计学差异,但SEMS组的临床成功率显著高于TADT组(p = 0.0040)。关于根治性手术后的术后并发症,SEMS组的并发症(≥2级)显著低于手术组(p = 0.022)。
接受OLCRC的SEMS置入术的患者与接受急诊手术的患者具有相似的肿瘤学结局。