Department of Pediatrics and Human Development, College of Human Medicine, Michigan State University, Grand Rapids, MI 49503, USA; Department of Pharmacology and Toxicology, College of Human Medicine, Michigan State University, Grand Rapids, MI 49503, USA.
Department of Pediatrics and Human Development, College of Human Medicine, Michigan State University, Grand Rapids, MI 49503, USA; Pediatric Intensive Care Unit, Helen DeVos Children's Hospital, 100 Michigan Street NE, Grand Rapids, MI 49503, USA.
EBioMedicine. 2020 Dec;62:103122. doi: 10.1016/j.ebiom.2020.103122. Epub 2020 Nov 25.
Multiple organ dysfunction syndrome (MODS) occurs in the setting of a variety of pathologies including infection and trauma. Some patients decompensate and require Veno-Arterial extra corporeal membrane oxygenation (ECMO) as a palliating manoeuvre for recovery of cardiopulmonary function. The molecular mechanisms driving progression from MODS to cardiopulmonary collapse remain incompletely understood, and no biomarkers have been defined to identify those MODS patients at highest risk for progression to requiring ECMO support.
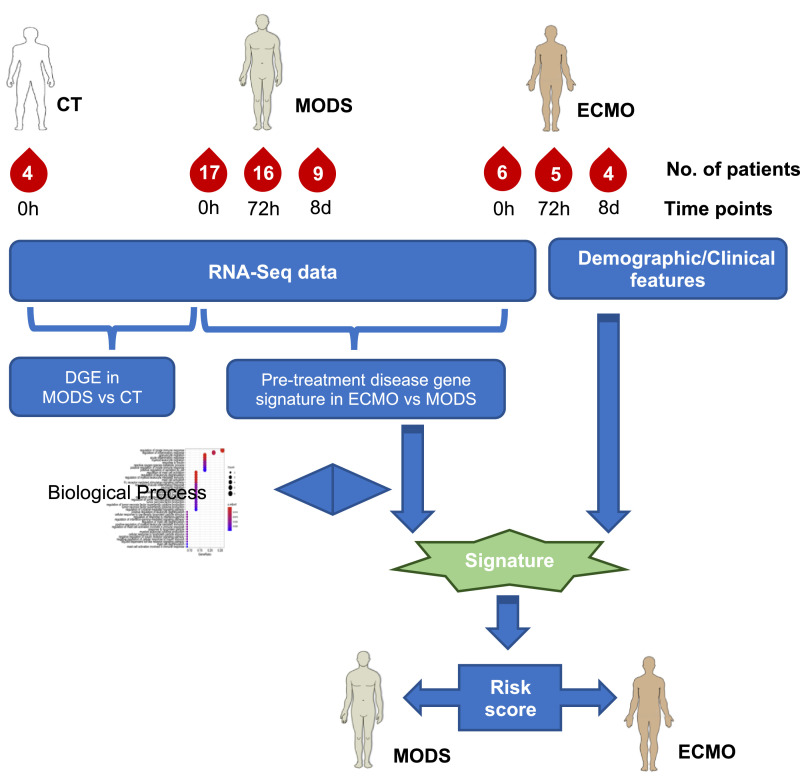
Whole blood RNA-seq profiling was performed for 23 MODS patients at three time points during their ICU stay (at diagnosis of MODS, 72 hours after, and 8 days later), as well as four healthy controls undergoing routine sedation. Of the 23 MODS patients, six required ECMO support (ECMO patients). The predictive power of conventional demographic and clinical features was quantified for differentiating the MODS and ECMO patients. We then compared the performance of markers derived from transcriptomic profiling including [1] transcriptomically imputed leukocyte subtype distribution, [2] relevant published gene signatures and [3] a novel differential gene expression signature computed from our data set. The predictive power of our novel gene expression signature was then validated using independently published datasets.
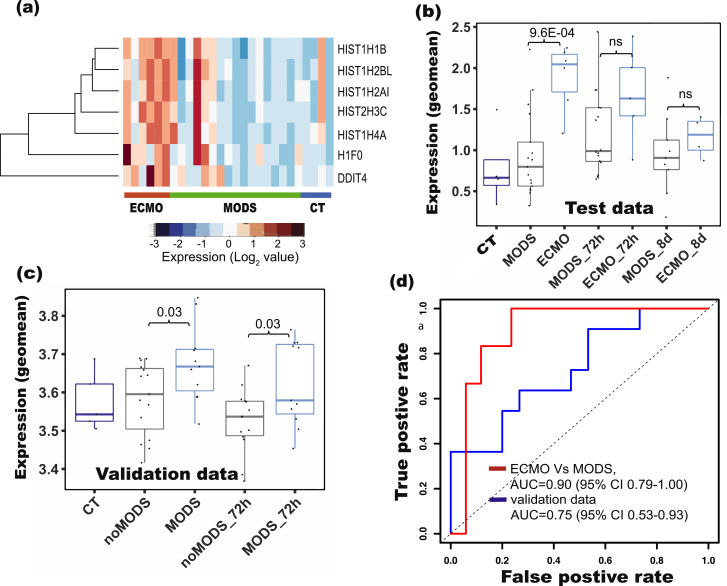
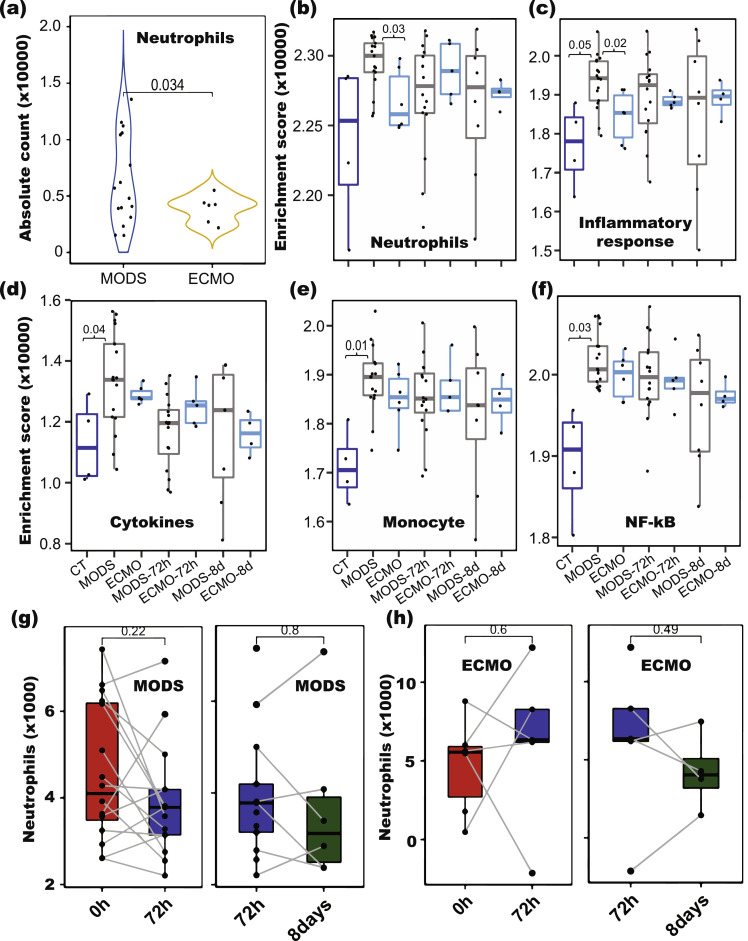
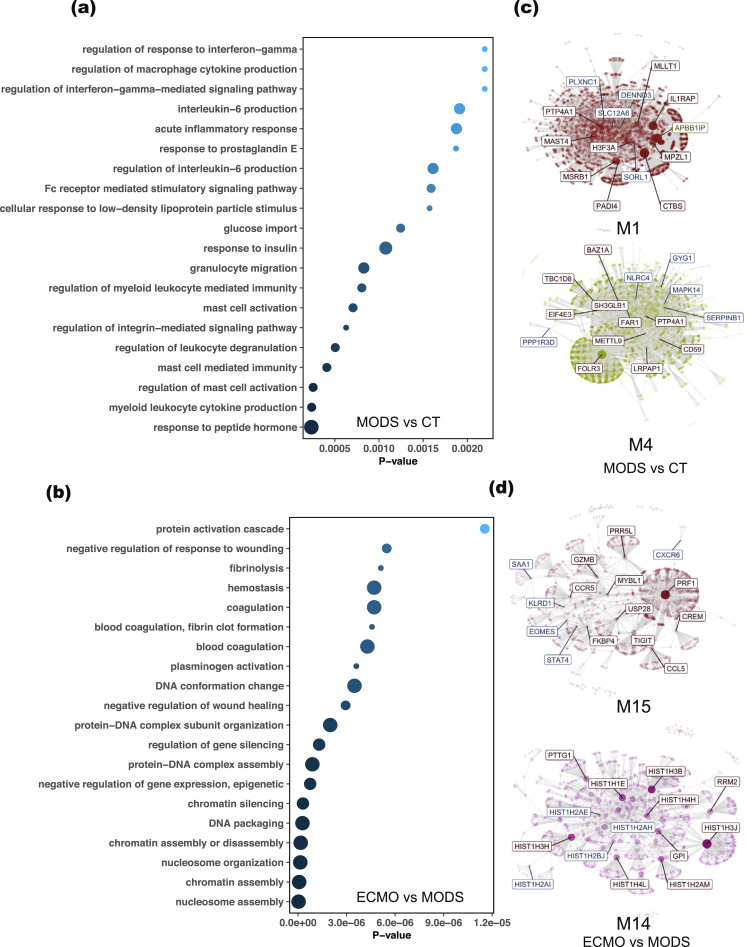
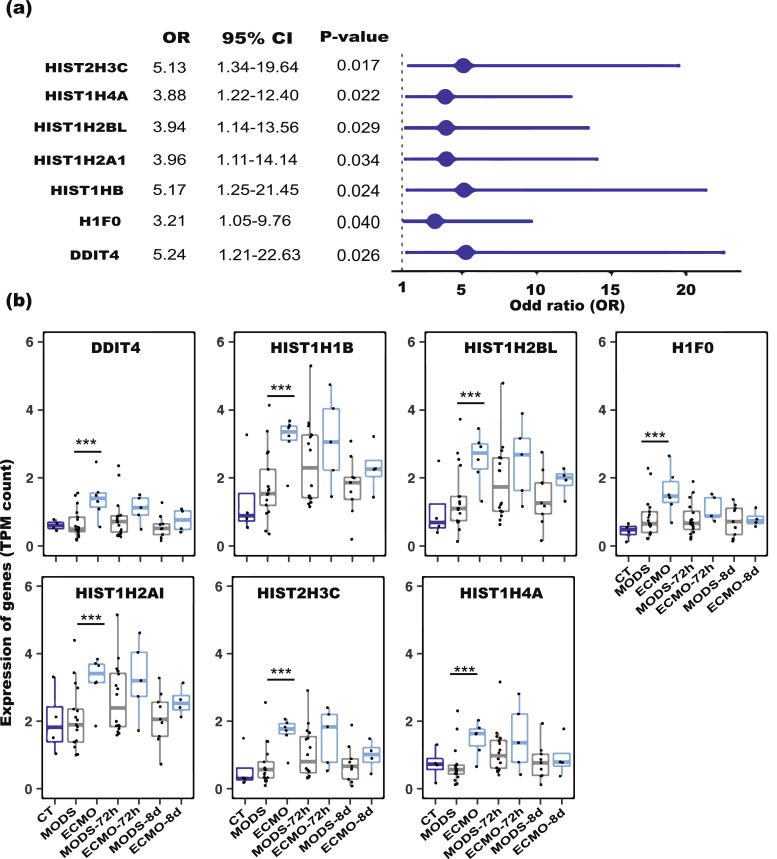
None of the five demographic characteristics and 14 clinical features, including The Paediatric Logistic Organ Dysfunction (PELOD) score, could predict deterioration of MODS to ECMO at baseline. From previously published sepsis signatures, only the signatures positively associated with patient's mortality could differentiate ECMO patients from MODS patients, when applied to our transcriptomic dataset (P-value ranges from 0.01 to 0.04, Student's test). Deconvolution of bulk RNA-Seq samples suggested that lower neutrophil counts were associated with increased risk of progression from MODS to ECMO (P-value = 0.03, logistic regression, OR=2.82 [95% CI 0.63 - 12.45]). A total of 30 genes were differentially expressed between ECMO and MODS patients at baseline (log2 fold change ≥ 1 or ≤ -1 with false discovery rate ≤ 0.01). These genes are involved in protein maintenance and epigenetic-related processes. Further univariate analysis of these 30 genes suggested a signature of seven DE genes associated with ECMO (OR > 3.0, P-value ≤ 0.05, logistic regression). Notably, this contains a set of histone marker genes, including H1F0, HIST2H3C, HIST1H2AI, HIST1H4, HIST1H2BL and HIST1H1B, that were highly expressed in ECMO. A risk score derived from expression of these genes differentiated ECMO and MODS patients in our dataset (AUC = 0.91, 95% CI 0.79-1.00, P-value = 7e-04, logistic regression) as well as validation dataset (AUC= 0.73, 95% CI 0.53-0.93, P-value = 2e-02, logistic regression).
This study demonstrates that transcriptomic features can serve as indicators of severity that could be superior to traditional methods of ascertaining acuity in MODS patients. Analysis of expression of signatures identified in this study could help clinicians in the diagnosis and prognostication of MODS patients after arrival to the Hospital.
多器官功能障碍综合征(MODS)发生在多种病理情况下,包括感染和创伤。一些患者失代偿并需要静脉-动脉体外膜肺氧合(ECMO)作为心肺功能恢复的姑息性治疗。从 MODS 进展为心肺衰竭的分子机制仍不完全清楚,也没有生物标志物来识别那些 MODS 患者最有可能需要 ECMO 支持。
对 23 名 MODS 患者在 ICU 住院期间的三个时间点(MODS 诊断时、72 小时后和 8 天后)以及 4 名接受常规镇静的健康对照者进行全血 RNA-seq 分析。在 23 名 MODS 患者中,有 6 名需要 ECMO 支持(ECMO 患者)。量化了常规人口统计学和临床特征对区分 MODS 和 ECMO 患者的预测能力。然后,我们比较了来自转录组分析的标志物的性能,包括[1]转录推断的白细胞亚型分布,[2]相关的已发表基因特征和[3]从我们的数据集中计算出的新的差异基因表达特征。然后使用独立发表的数据集验证我们新的基因表达特征的预测能力。
在基线时,五种人口统计学特征和 14 种临床特征,包括儿科逻辑器官功能障碍(PELOD)评分,都不能预测 MODS 恶化到 ECMO。从先前发表的败血症特征中,只有与患者死亡率正相关的特征可以将 ECMO 患者与 MODS 患者区分开来,当应用于我们的转录组数据集时(P 值范围为 0.01 至 0.04,学生检验)。对批量 RNA-Seq 样本的去卷积表明,中性粒细胞计数较低与从 MODS 进展到 ECMO 的风险增加相关(P 值=0.03,逻辑回归,OR=2.82 [95%CI 0.63-12.45])。基线时 ECMO 和 MODS 患者之间有 30 个基因差异表达(log2 倍数变化≥1 或≤-1,假发现率≤0.01)。这些基因参与蛋白质维持和表观遗传相关过程。对这 30 个基因的进一步单变量分析表明,有 7 个 DE 基因与 ECMO 相关的特征(OR>3.0,P 值≤0.05,逻辑回归)。值得注意的是,这包含一组组蛋白标记基因,包括 H1F0、HIST2H3C、HIST1H2AI、HIST1H4、HIST1H2BL 和 HIST1H1B,它们在 ECMO 中高度表达。这些基因的表达衍生的风险评分可以区分我们数据集(AUC=0.91,95%CI 0.79-1.00,P 值=7e-04,逻辑回归)和验证数据集(AUC=0.73,95%CI 0.53-0.93,P 值=2e-02,逻辑回归)中的 ECMO 和 MODS 患者。
这项研究表明,转录组特征可以作为严重程度的指标,这可能优于传统的确定 MODS 患者严重程度的方法。分析本研究中确定的特征的表达可以帮助临床医生对到达医院后的 MODS 患者进行诊断和预后。