Department of Physiology & Biophysics, University of Mississippi Medical Center, 2500 North State Street, Jackson, MS 30216-4505, USA.
Mississippi Center for Obesity Research, University of Mississippi Medical Center, 2500 North State Street, Jackson, MS 30216-4505, USA.
Cardiovasc Res. 2021 Jul 7;117(8):1859-1876. doi: 10.1093/cvr/cvaa336.
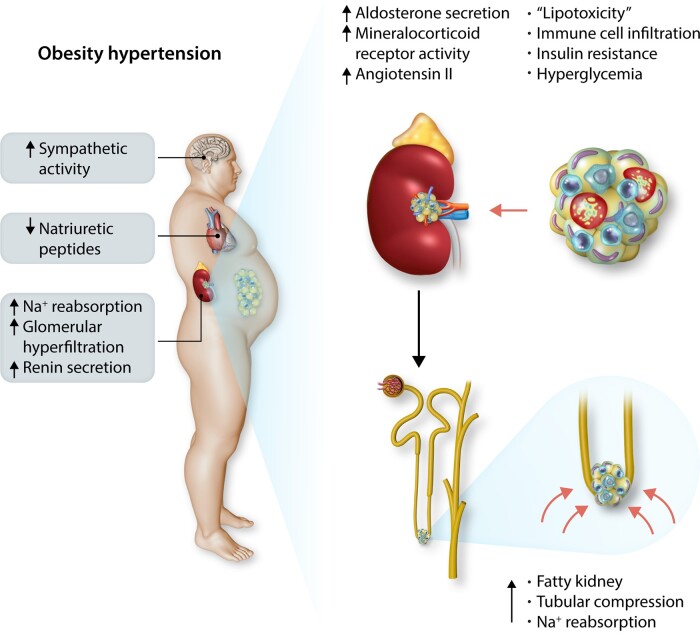
Obesity contributes 65-75% of the risk for human primary (essential) hypertension (HT) which is a major driver of cardiovascular and kidney diseases. Kidney dysfunction, associated with increased renal sodium reabsorption and compensatory glomerular hyperfiltration, plays a key role in initiating obesity-HT and target organ injury. Mediators of kidney dysfunction and increased blood pressure include (i) elevated renal sympathetic nerve activity (RSNA); (ii) increased antinatriuretic hormones such as angiotensin II and aldosterone; (iii) relative deficiency of natriuretic hormones; (iv) renal compression by fat in and around the kidneys; and (v) activation of innate and adaptive immune cells that invade tissues throughout the body, producing inflammatory cytokines/chemokines that contribute to vascular and target organ injury, and exacerbate HT. These neurohormonal, renal, and inflammatory mechanisms of obesity-HT are interdependent. For example, excess adiposity increases the adipocyte-derived cytokine leptin which increases RSNA by stimulating the central nervous system proopiomelanocortin-melanocortin 4 receptor pathway. Excess visceral, perirenal and renal sinus fat compress the kidneys which, along with increased RSNA, contribute to renin-angiotensin-aldosterone system activation, although obesity may also activate mineralocorticoid receptors independent of aldosterone. Prolonged obesity, HT, metabolic abnormalities, and inflammation cause progressive renal injury, making HT more resistant to therapy and often requiring multiple antihypertensive drugs and concurrent treatment of dyslipidaemia, insulin resistance, diabetes, and inflammation. More effective anti-obesity drugs are needed to prevent the cascade of cardiorenal, metabolic, and immune disorders that threaten to overwhelm health care systems as obesity prevalence continues to increase.
肥胖导致人类原发性(特发性)高血压(HT)的风险占 65-75%,而 HT 是心血管和肾脏疾病的主要驱动因素。肾脏功能障碍与肾钠重吸收增加和代偿性肾小球高滤过有关,在引发肥胖-HT 和靶器官损伤中起着关键作用。肾脏功能障碍和血压升高的介质包括:(i)升高的肾交感神经活动(RSNA);(ii)增加的抗利尿激素,如血管紧张素 II 和醛固酮;(iii)相对缺乏利钠激素;(iv)肾脏周围和内部脂肪对肾脏的压迫;(v)固有和适应性免疫细胞的激活,这些细胞会侵入全身组织,产生炎症细胞因子/趋化因子,导致血管和靶器官损伤,并使 HT 恶化。这些肥胖-HT 的神经激素、肾脏和炎症机制是相互依存的。例如,过多的脂肪会增加脂肪细胞衍生的细胞因子瘦素,通过刺激中枢神经系统 proopiomelanocortin-melanocortin 4 受体途径来增加 RSNA。过多的内脏、肾周和肾窦脂肪会压迫肾脏,加上 RSNA 的增加,会导致肾素-血管紧张素-醛固酮系统的激活,尽管肥胖也可能独立于醛固酮激活盐皮质激素受体。长期肥胖、HT、代谢异常和炎症会导致进行性肾脏损伤,使 HT 更难治疗,通常需要多种降压药物,同时治疗血脂异常、胰岛素抵抗、糖尿病和炎症。需要更有效的抗肥胖药物来预防心血管、代谢和免疫紊乱的级联反应,因为肥胖的流行继续增加,这可能会使医疗保健系统不堪重负。