van Delft Brenda, Van Ginderdeuren Filip, Lefevere Julie, van Delft Christel, Cools Filip
Neonatology, UZ Brussel, Brussels, Belgium.
Rehabilitation Research, Department of Physiotherapy, UZ Brussel, Brussels, Belgium.
BMJ Paediatr Open. 2020 Nov 19;4(1):e000858. doi: 10.1136/bmjpo-2020-000858. eCollection 2020.
The optimal method to wean preterm infants from non-invasive respiratory support (NIVRS) with nasal continuous positive airway pressure (CPAP) or high-flow nasal cannula is still unclear, and methods used vary considerably between neonatal units.
Perform a systematic review and meta-analysis to determine the most effective strategy for weaning preterm infants born before 37 weeks' gestation from NIVRS.
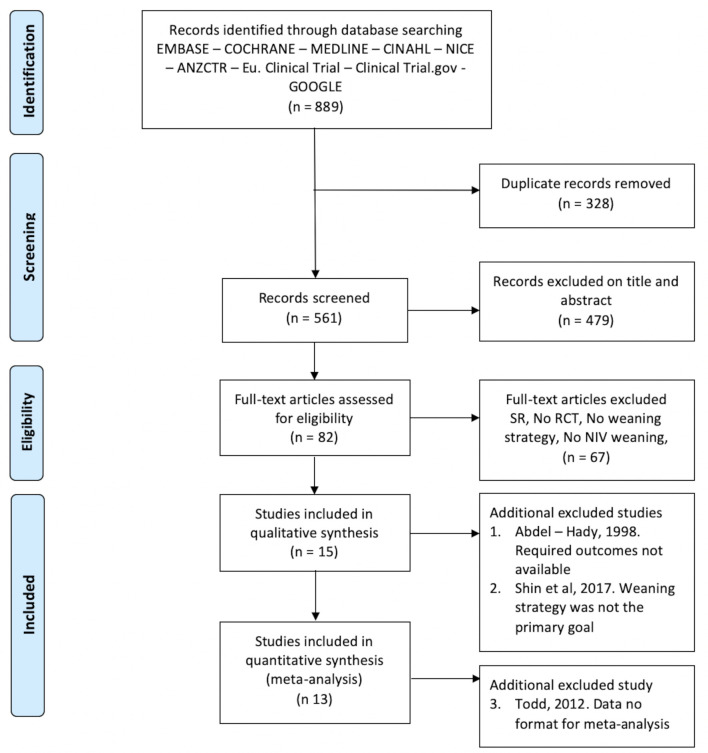
EMBASE, MEDLINE, CINAHL, Google and Cochrane Central Register of Controlled Trials were searched for randomised controlled trials comparing different weaning strategies of NIVRS in infants born before 37 weeks' gestation.
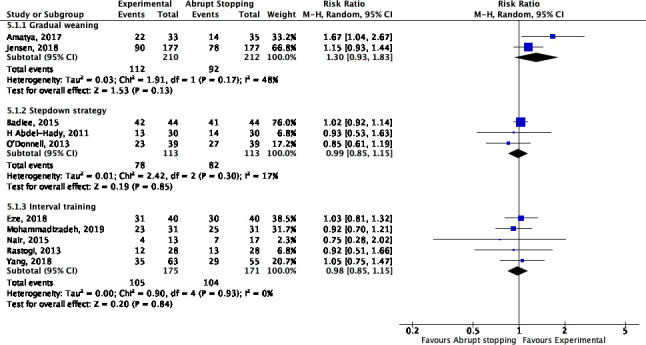
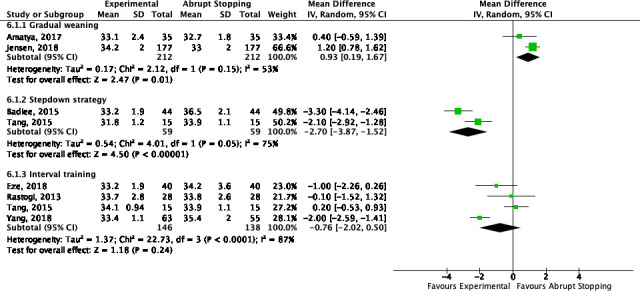
Fifteen trials (1.547 infants) were included. With gradual pressure wean, the relative risk of successful weaning at the first attempt was 1.30 (95% CI 0.93 to 1.83), as compared with sudden discontinuation. Infants were weaned at a later postmenstrual age (PMA) (median difference (MD) 0.93 weeks (95% CI 0.19 to 1.67)). A stepdown strategy to nasal cannula resulted in an almost 3-week reduction in the PMA at successful weaning (MD -2.70 (95% CI -3.87 to -1.52)) but was associated with a significantly longer duration of oxygen supplementation (MD 7.80 days (95% CI 5.31 to 10.28)). A strategy using interval training had no clinical benefits. None of the strategies had any effect on the risk of chronic lung disease or the duration of hospital stay.
A strategy of gradual weaning of airway pressure might increase the chances of successful weaning. Stepdown strategy from CPAP to nasal cannula is a useful alternative resulting in an earlier weaning, but the focus should remain on continued weaning in order to avoid prolonged oxygen supplementation. Interval training should probably not be used.
对于孕周小于37周的早产婴儿,采用鼻持续气道正压通气(CPAP)或高流量鼻导管进行无创呼吸支持撤机的最佳方法仍不明确,且不同新生儿病房所采用的方法差异很大。
进行系统评价和荟萃分析,以确定孕周小于37周的早产婴儿无创呼吸支持撤机的最有效策略。
检索EMBASE、MEDLINE、CINAHL、谷歌以及Cochrane对照试验中心注册库,查找比较孕周小于37周婴儿无创呼吸支持不同撤机策略的随机对照试验。
纳入15项试验(1547例婴儿)。与突然停止相比,采用逐渐降低压力撤机,首次尝试成功撤机的相对风险为1.30(95%置信区间0.93至1.83)。婴儿在更大的月经后年龄(PMA)撤机(中位数差值(MD)0.93周(95%置信区间0.19至1.67))。采用逐步降低至鼻导管的策略,成功撤机时PMA几乎缩短3周(MD -2.70(95%置信区间 -3.87至 -1.52)),但与吸氧持续时间显著延长有关(MD 7.80天(95%置信区间5.31至10.28))。采用间歇训练的策略无临床益处。这些策略均对慢性肺病风险或住院时间无影响。
气道压力逐渐降低的撤机策略可能会增加成功撤机的机会。从CPAP逐步降低至鼻导管的策略是一种有用的替代方法,可实现更早撤机,但应继续关注撤机过程,以避免吸氧时间延长。间歇训练可能不应采用。