Division of Hematology and Oncology Medicine, Department of Internal Medicine, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan (R.O.C.).
Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan (R.O.C.).
PLoS One. 2020 Dec 2;15(12):e0242900. doi: 10.1371/journal.pone.0242900. eCollection 2020.
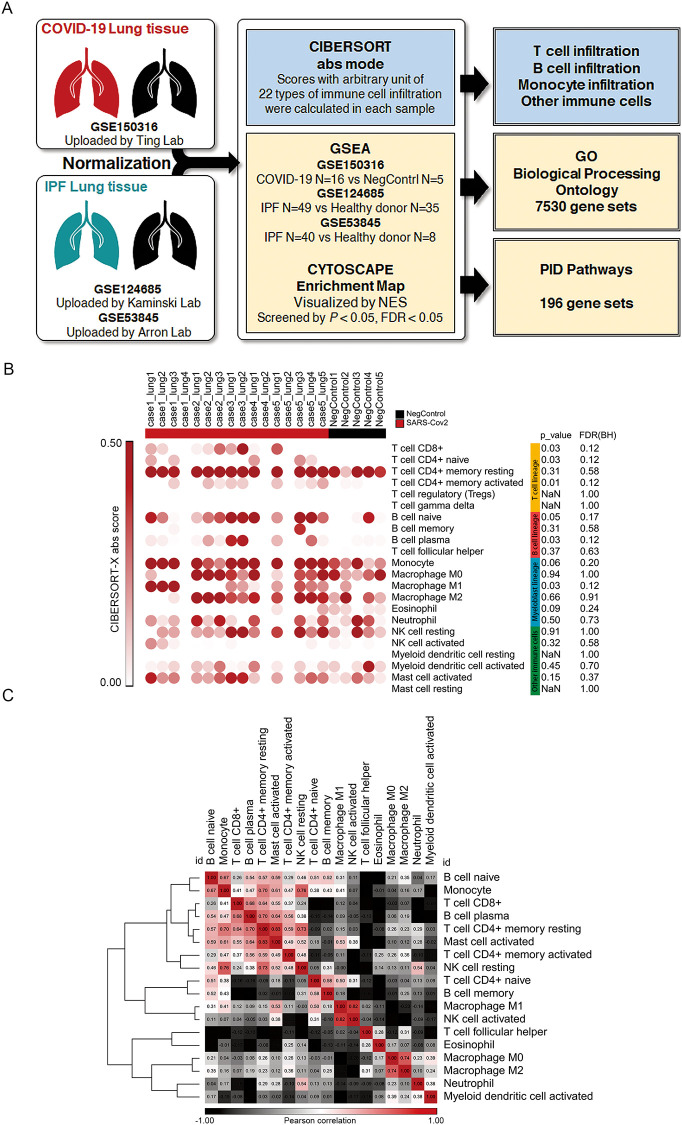
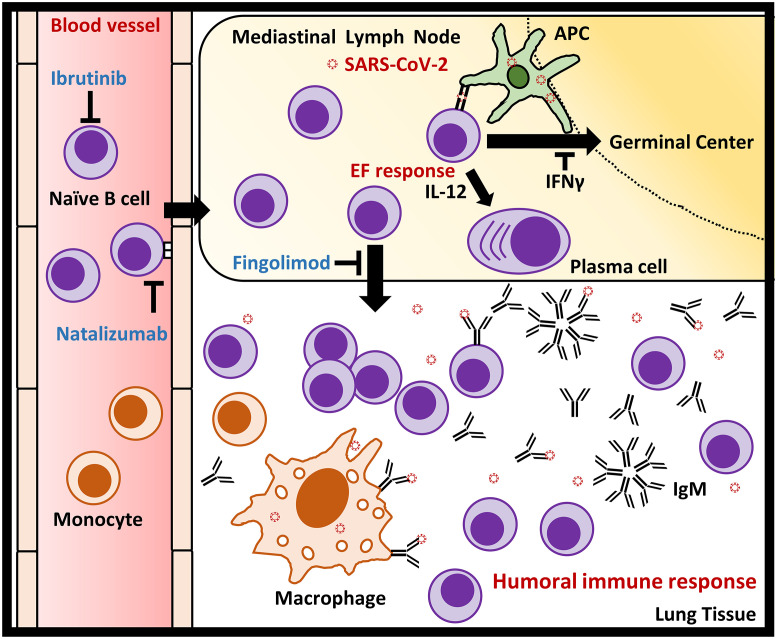
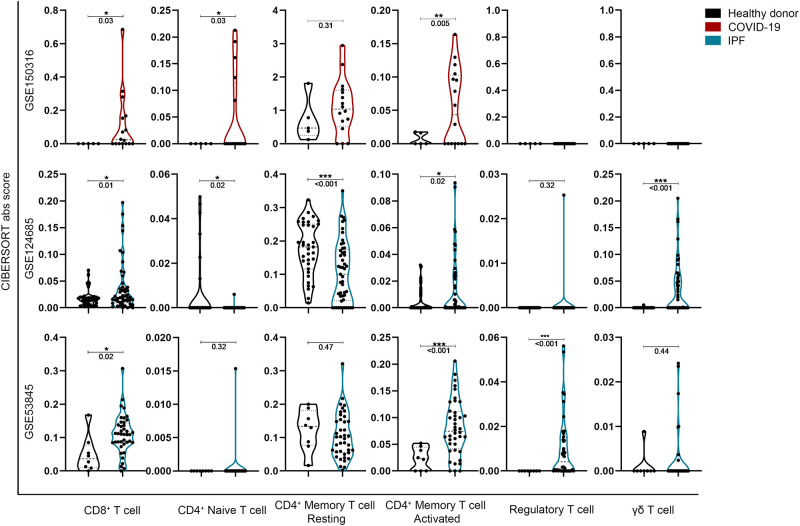
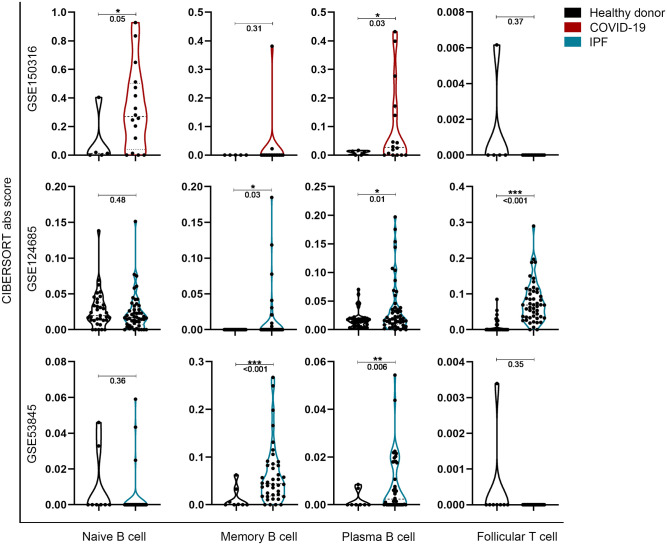
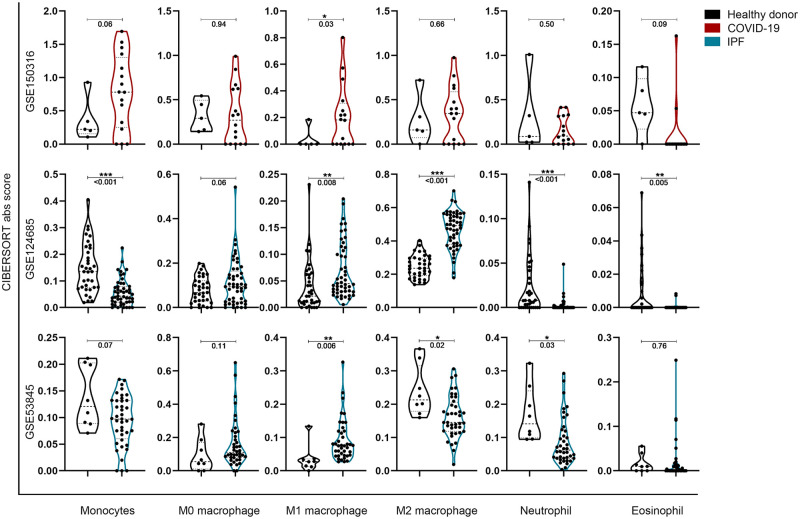
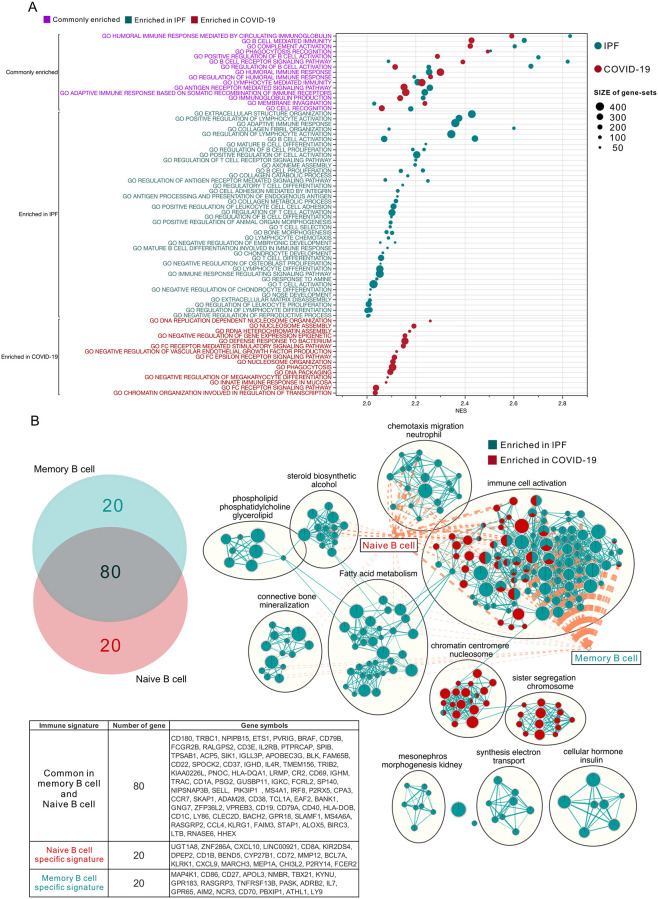
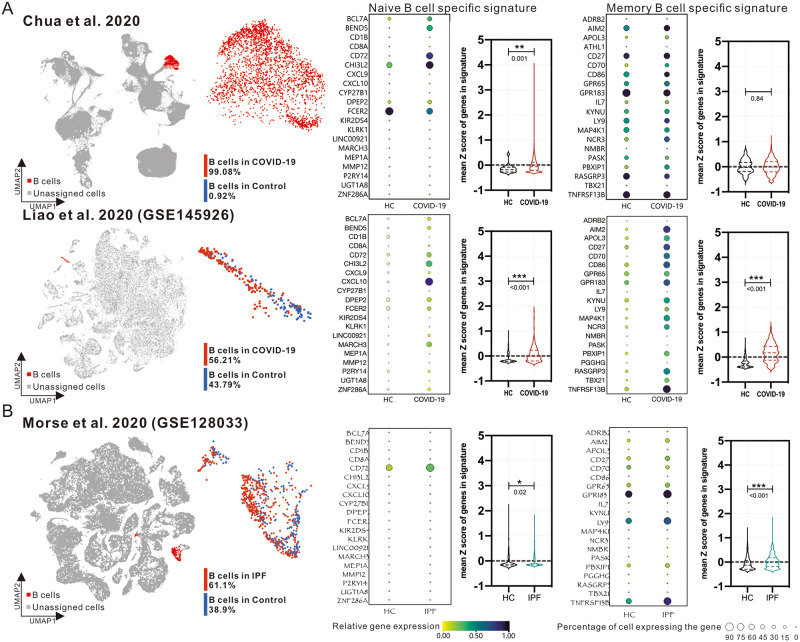
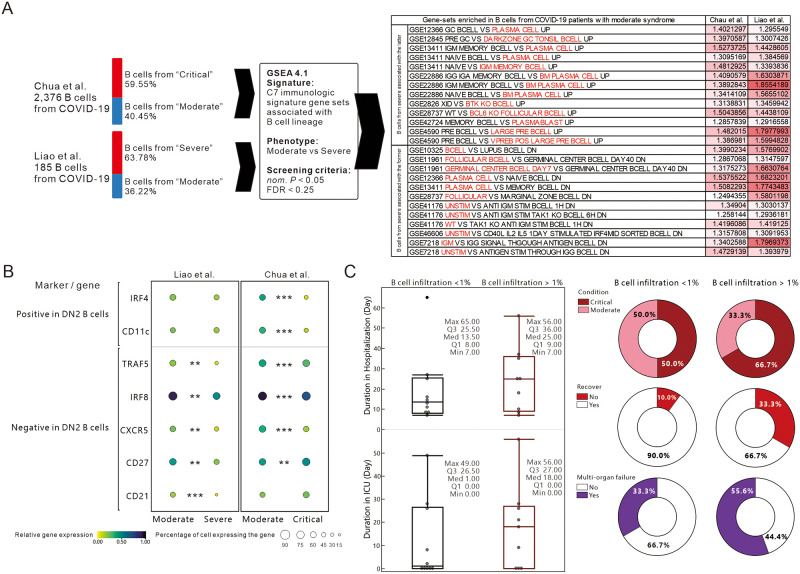
COVID-19, caused by SARS-CoV-2, has rapidly spread to more than 160 countries worldwide since 2020. Despite tremendous efforts and resources spent worldwide trying to explore antiviral drugs, there is still no effective clinical treatment for COVID-19 to date. Approximately 15% of COVID-19 cases progress to pneumonia, and patients with severe pneumonia may die from acute respiratory distress syndrome (ARDS). It is believed that pulmonary fibrosis from SARS-CoV-2 infection further leads to ARDS, often resulting in irreversible impairment of lung function. If the mechanisms by which SARS-CoV-2 infection primarily causes an immune response or immune cell infiltration can be identified, it may be possible to mitigate excessive immune responses by modulating the infiltration and activation of specific targets, thereby reducing or preventing severe lung damage. However, the extent to which immune cell subsets are significantly altered in the lung tissues of COVID-19 patients remains to be elucidated. This study applied the CIBERSORT-X method to comprehensively evaluate the transcriptional estimated immune infiltration landscape in the lung tissues of COVID-19 patients and further compare it with the lung tissues of patients with idiopathic pulmonary fibrosis (IPF). We found a variety of immune cell subtypes in the COVID-19 group, especially naïve B cells were highly infiltrated. Comparison of functional transcriptomic analyses revealed that non-differentiated naïve B cells may be the main cause of the over-active humoral immune response. Using several publicly available single-cell RNA sequencing data to validate the genetic differences in B-cell populations, it was found that the B-cells collected from COVID-19 patients were inclined towards naïve B-cells, whereas those collected from IPF patients were inclined towards memory B-cells. Further differentiation of B cells between COVID-19 mild and severe patients showed that B cells from severe patients tended to be antibody-secreting cells, and gene expression showed that B cells from severe patients were similar to DN2 B cells that trigger extrafollicular response. Moreover, a higher percentage of B-cell infiltration seems associated with poorer clinical outcome. Finally, a comparison of several specific COVID-19 cases treated with targeted B-cell therapy suggests that appropriate suppression of naïve B cells might potentially be a novel strategy to alleviate the severe symptoms of COVID-19.
自 2020 年以来,由严重急性呼吸综合征冠状病毒 2 (SARS-CoV-2)引起的 COVID-19 已迅速传播到全球 160 多个国家。尽管全世界都在努力探索抗病毒药物,但迄今为止,仍然没有针对 COVID-19 的有效临床治疗方法。大约 15%的 COVID-19 病例进展为肺炎,重症肺炎患者可能死于急性呼吸窘迫综合征(ARDS)。据信,SARS-CoV-2 感染引起的肺纤维化进一步导致 ARDS,通常导致肺功能不可逆转的损害。如果能够确定 SARS-CoV-2 感染主要引起免疫反应或免疫细胞浸润的机制,那么通过调节特定靶标的浸润和激活,减轻过度的免疫反应,从而减少或预防严重的肺损伤,可能是可行的。然而,COVID-19 患者肺组织中免疫细胞亚群的改变程度仍有待阐明。本研究应用 CIBERSORT-X 方法全面评估 COVID-19 患者肺组织中的转录估计免疫浸润图谱,并与特发性肺纤维化(IPF)患者的肺组织进行比较。我们在 COVID-19 组中发现了多种免疫细胞亚型,特别是幼稚 B 细胞高度浸润。功能转录组分析比较显示,未分化的幼稚 B 细胞可能是过度活跃的体液免疫反应的主要原因。使用几种公开可用的单细胞 RNA 测序数据来验证 B 细胞群体的遗传差异,发现从 COVID-19 患者中采集的 B 细胞倾向于幼稚 B 细胞,而从 IPF 患者中采集的 B 细胞则倾向于记忆 B 细胞。进一步区分 COVID-19 轻症和重症患者的 B 细胞,发现重症患者的 B 细胞倾向于成为抗体分泌细胞,基因表达显示重症患者的 B 细胞类似于触发滤泡外反应的 DN2 B 细胞。此外,较高的 B 细胞浸润百分比似乎与较差的临床结果相关。最后,对几种特定的 COVID-19 病例进行靶向 B 细胞治疗的比较表明,适当抑制幼稚 B 细胞可能是缓解 COVID-19 严重症状的一种新策略。