Povlsen Jonas Agerlund, Rasmussen Vibeke Guldbrand, Vase Henrik, Jensen Kaare Troels, Terkelsen Christian Juhl, Christiansen Evald Høj, Tang Mariann, Pedersen Anders Lehmann Dahl, Poulsen Steen Hvitfeldt
Department of Cardiology, Aarhus University Hospital, Palle Juul-Jensens Boulevard 99, 8200, Aarhus N, Denmark.
Department of Cardiothoracic Surgery, Aarhus University Hospital, Palle Juul-Jensens Boulevard 99, 8200, Aarhus N, Denmark.
BMC Cardiovasc Disord. 2020 Dec 2;20(1):506. doi: 10.1186/s12872-020-01791-9.
The aim of present study was to examine the preoperative prevalence and distribution of impaired left ventricular global longitudinal strain (LVGLS) in elderly patients with symptomatic aortic stenosis (AS) undergoing transcutaneous aortic valve replacement (TAVR) and to determine the predictive value of LVGLS on survival.
We included 411 patients with symptomatic severe AS treated with TAVR during a 5-year period, where a baseline echocardiography including LVGLS assessment was available.
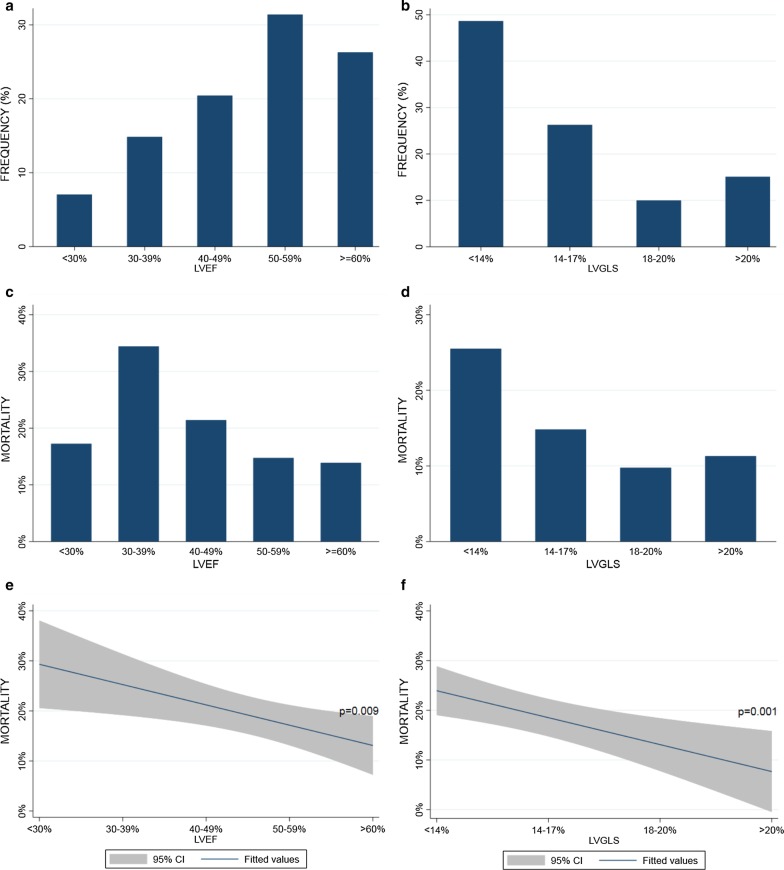
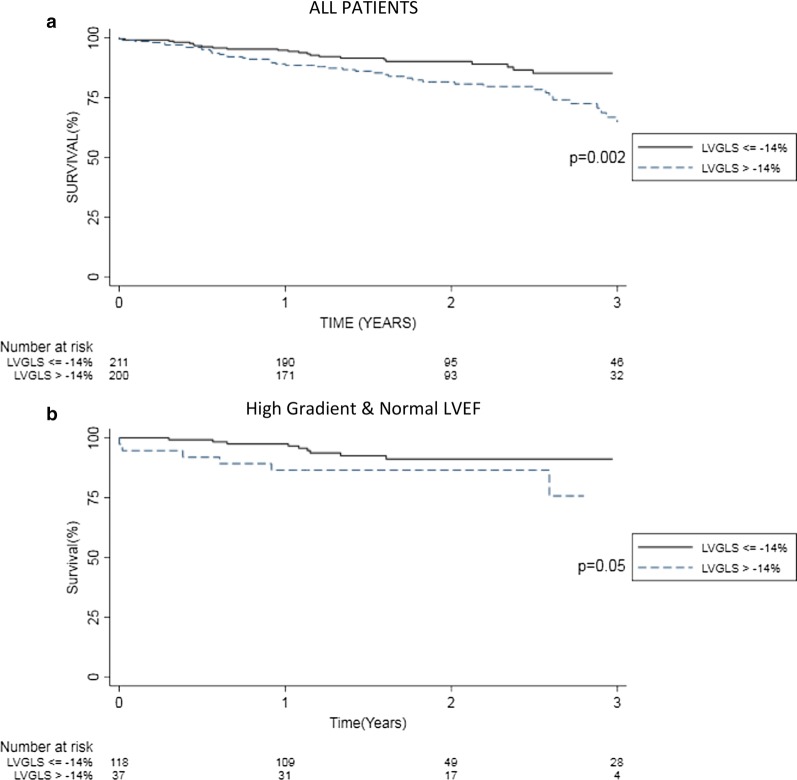
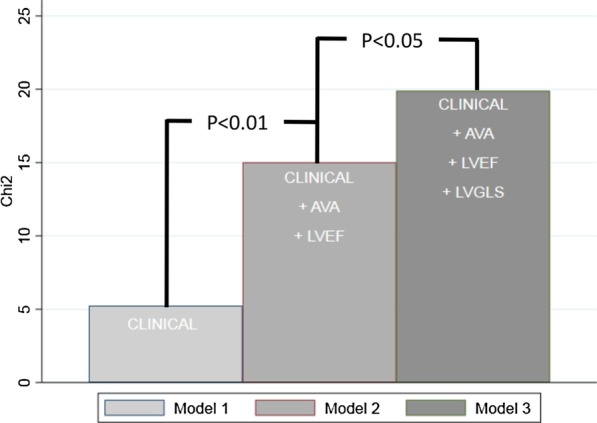
Mean age was 80.1 ± 7.1 years and aortic valve area (AVA) index 0.4 ± 0.1 cm. 78 patients died during a median follow-up of 762 days. Mean left ventricular ejection fraction (LVEF) was 50 ± 13% and mean LVGLS was - 14.0%. LVEF was preserved in 60% of patients, while impaired LVGLS > - 18% was seen in 75% of the patients. Previous myocardial infarction, LVEF < 50%, LVGLS > - 14%, low gradient AS (< 4.0 m/s), tricuspid regurgitant gradient > 30 mmHg were identified as significant univariate predictors of all-cause mortality. On multivariate analysis LVGLS > - 14% (HR 1.79 [1.02-3.14], p = 0.04) was identified as the only independent variable associated with all-cause mortality. Reduced survival was observed with an impaired LVGLS > - 14% in the total population (p < 0.002) but also in patients with high AS gradient with preserved LVEF. LVGLS provided incremental prognostic value with respect to clinical characteristics, AVA and LVEF (χ 19.9, p = 0.006).
In patients with symptomatic AS undergoing TAVR, impaired LVGLS was highly prevalent despite preserved LVEF. LVGLS > - 14% was an independent predictor of all-cause mortality, and survival was reduced if LVGLS > - 14%.
本研究旨在探讨接受经皮主动脉瓣置换术(TAVR)的有症状主动脉瓣狭窄(AS)老年患者术前左心室整体纵向应变(LVGLS)受损的患病率及分布情况,并确定LVGLS对生存率的预测价值。
我们纳入了411例在5年期间接受TAVR治疗的有症状重度AS患者,这些患者均有包括LVGLS评估的基线超声心动图检查资料。
平均年龄为80.1±7.1岁,主动脉瓣面积(AVA)指数为0.4±0.1cm²。在中位随访762天期间,78例患者死亡。平均左心室射血分数(LVEF)为50±13%,平均LVGLS为-14.0%。60%的患者LVEF正常,而75%的患者LVGLS受损>-18%。既往心肌梗死、LVEF<50%、LVGLS>-14%、低跨瓣压差AS(<4.0m/s)、三尖瓣反流压差>30mmHg被确定为全因死亡率的显著单因素预测指标。多因素分析显示,LVGLS>-14%(HR 1.79[1.02-3.14],p=0.04)是与全因死亡率相关的唯一独立变量。在总体人群中,LVGLS>-14%时生存率降低(p<0.002),在AS跨瓣压差高且LVEF正常的患者中也是如此。LVGLS相对于临床特征、AVA和LVEF具有增量预后价值(χ²=19.9,p=0.006)。
在接受TAVR的有症状AS患者中,尽管LVEF正常,但LVGLS受损仍很常见。LVGLS>-14%是全因死亡率的独立预测指标,若LVGLS>-14%则生存率降低。